Download

1 / 25
260 likes | 367 Views
DEPRESSION. By, Vishal Patel Tehreema Jaffar. INTRODUCTION and EPIDEMIOLOGY.

E N D
DEPRESSION By, Vishal Patel Tehreema Jaffar
INTRODUCTION and EPIDEMIOLOGY • Depression refers to a wide variety of abnormal variations in an individual's mood. Individuals with mood disorders experience extremes of emotions(eg. Sadness) that are higher in intensity and longer in duration than normal. • The Diagnostic and Statistical Manual of Mental Disorders (DSM) states that a depressed mood is often reported as feeling sad, helpless, and hopeless. • WHO estimates that approx 450 million people throughout the world struggle with a mental health problem. Depression is a major category of mental health distress affecting people of every age, background and ethnicity.
Depression is the leading cause of disability as measured by years lived with disability • and is the 4th leading contributor to the global burden of disease in 2000. • < 25 % of those affected have access to effective treatments. • At its worst, depression can lead to suicide, a tragic fatality associated with the loss of about 850 000 thousand lives every year. • About 2 in 3 adults suffer from depression at some time in their life. An episode of depression serious enough to require treatment occurs in about 1 in 4 women and 1 in 10 men.
Depressive illness occurs in 2-4% of children (Rare if < 8yrs old). • It becomes more common after puberty + more frequently in girls. • Adolescents may seem irritable rather than sad, which can be confusing, particularly if the young person withdraws and shuts themselves away. • Depressed children and adolescents often have other psychiatric problems as well, such as behaviour problems or anxiety. As a result, they may get in fights or other trouble at school, interact less socially and lose friends.
Depression, anxiety and other forms of mental illness have taken over from unemployment as the greatest social problem in the UK.Around 15% of the population suffers from depression or anxiety, and the effects on home, career, relationships and personal esteem are enormous. • There are now more than 1million mentally ill people receiving incapacity benefits - more than the total number of unemployed people receiving unemployment benefits. • WHO predicts depression will be the second leading cause of death by 2020. Many blame increasing job and relationship insecurity for the rise in mental illness.
Depression amongst the famous • A recent study examined the lives of 300 famous people and found that highest rates of depression (72%) were found in writers, but the incidence was also high in artists (42%), politicians (41%), intellectuals (36%), composers (35%), and scientists (33%). • Famous people who have publicly stated they have had a depressive illness include: • Anthony Hopkins, actor • Barbara Bush, former First Lady (U.S.) • Elton John, musician, composer • Halle Berry, actress • Harrison Ford, actor • Janet Jackson, musician • Jim Carrey, actor, comedian • Yves Saint Laurent, fashion designer
SYMPTOMS • Although the terminology is slightly different between ICD-10 (used in Europe) and DSM-IV (America), the core symptoms for depression are almost identical, and should fulfil the following criteria: • Present for at least 2 weeks and represent a change from normal. • Are not secondary to the effects of drug/alcohol misuse, medication, a medical disorder, or bereavement. • May cause significant distress and/or impairment of social, occupational, or general functioning. • Features: • 1. Lowered mood • 2. Reduced energy levels • 3. Deceased activity levels • And at least 4 of the following (‘somatic’ or biological symptoms): • 4. Loss of interest in normally enjoyable activities (‘anhedonia’) • 5. Decrease of or lack of emotional reactions to events that would usually elicit a reaction. • 6. Early morning waking from sleep (2 or more hours before usual time) • 7. Mood worse in the morning (diurnal mood variation) • 8. Objective evidence of psychomotor agitation or retardation • 9. Loss of appetite • 10. Weight loss (at least 5% of body weight over the previous month) • 11. Loss of libido (sex drive)
Psychotic symptoms: • Delusions: e.g. poverty; personal inadequacy; guilt over presumed misdeeds; responsibility for world events: accidents, natural disasters, war.Hallucinations:Auditory: accusatory voices, cries for help or screaming. Olfactory: bad smells such as rotting food, faeces, decomposing flesh. Visual: tormentors, demons, the Devil, dead bodies, scenes of death or torture. • Catatonic symptoms or marked psychomotor retardation (depressive stupor). Indirect presentations may include: • Elderly persons presenting with agitation, confusion, or a decline in normal functioning (pseudodementia). • Children presenting with symptoms such • as irritability, decline in school performance • , or social withdrawal.
Other forms of depression 1. Atypical depressive episode • Regarded as a subtype of depressive disorder, rather than a separate entity. • Mood is depressed but remains reactive (able to enjoy certain experiences but not to normal levels). • Hypersomnia (sleeping more than 10 hrs/day, at least 3 days/wk, for at least 3 months). • Hyperphagia (excessive eating with weight gain of over 3kg in 3 months). • Leaden paralysis (feeling of heaviness in the limbs, present for at least 1 hr/day, 3 days/wk, for at least 3 months). • Onset usually in late teens and early twenties. 2. Seasonal affective disorder (SAD) • There is a clear seasonal pattern to recurrent depressive episodes. In the northern hemisphere this is usually around January/ February (winter depression). Symptoms: low self-esteem, hypersomnia, fatigue, increased appetite (including carbohydrate craving) and weight gain. 3. Postnatal depression: • A significant depressive episode, related to childbirth, occurring in 10-15% of women, within 6 months post-partum. Content may include worries about the baby's health, or her ability to cope adequately with the baby. There may be a significant anxiety component. • 90% of cases last less than 1 month; 4% greater than one year.
Etiology of depression: • Risk factors: • Genetic Heritability: ranges from 40- 70 %, and families also have high rates of anxiety disorders and neuroticism. • Childhood experiences: Loss of a parent, lack of parental care, parental alcoholism, childhood sexual abuse. • Personality traits: anxiety, impulsivity, obsessions. • Social circumstances: • Marital status: (in men: high rates with separation or divorce; in women: probably similar but less clear-cut). • Women having 3 or more children under the age of 11, lack of paid employment, and lack of a confiding relationship are associated with increased risk of depression. • Adverse life events: particularly losses. Increased risk 2- 3 months after event in vulnerable individuals.
Physical illness: especially if chronic, severe, or painful. Higher rates noted in post-myocardial infarction, diabetic, and cancer patients. • Neurological disorders: Parkinson's disease, Multiple sclerosis, Stroke and Epilepsy have higher risk. Comorbidity: About two-thirds of patients will also suffer from another psychiatric disorder (e.g. anxiety disorders, substance misuse, alcohol dependency, personality disorders). • Neurobiological factors: Structural brain changes in chronic cases, especially left hippocampus, left parietal, and frontal association cortices. • Functional brain changes: Hypoperfusion in frontal, temporal, and parietal areas (especially older patients). Increased perfusion in frontal and cingulate cortex (in younger patients). • Neurotransmitter abnormalities: The discovery that all antidepressants increase monoamine release (i.e. Serotonin, Nor-epinephrine, Dopamine) and/or reduce their reuptake in the synaptic cleft, led to the development of the monoamine theory of depression. • Genetic factors: Linkage analysis suggests an association between the serotonin transporter gene (17q11) and depression.
Gender: • There is an increased prevalence of depression in women, and explanations for this are various. These include: restricting social and occupational roles, being over- or under-occupied, and endocrine factors (e.g. increased risk of depression in the premenstrual and post-partum periods). One popular hypothesis is that women are more likely to admit to depressive symptoms, whereas men are not, and tend to express their symptoms differently (e.g. through alcohol abuse and antisocial behaviour). Social factors: • People of low socio-economic status (i.e. low levels of income, employment, and education) are at a significantly higher risk of depression.
Diagnosis of depression: Laboratory investigations: • As there is no specific laboratory investigation for depression, • basic investigations should be guided by clinical presentation, and are aimed at ruling out obvious differential diagnoses.
Additionally, a number of non-routine investigations have been described in depression…
Differential diagnosis: • Other psychiatric disorders: Dysthymia, bipolar disorder, anxiety disorders, eating disorders, schizophrenia (negative symptoms), personality disorders. • Neurological disorders:Dementia, Parkinson's disease, Huntington's disease, MS, stroke, epilepsy. • Endocrine disorders: Addison's disease, Cushing's disease, hyper/ hypothyroidism, menopausal symptoms, hyperparathyroidism, hypopituitarism. • Metabolic disorders: Hypoglycaemia, hypercalcaemia, porphyria. • Infections: Syphilis, Lyme disease, and HIV encephalopathy. • Sleep disorders: Especially sleep apnoea. • Medication-related: Antihypertensives (beta-blockers, methyldopa, and calcium channel blockers); steroids; chemotherapy agents (e.g., vincristine, interferon, amphotericin B, vinblastine); medications that affect sex hormones (oestrogen, progesterone, testosterone); and psychiatric medication (esp. antipsychotics) • Substance misuse: Alcohol, benzodiazepines, opiates, marijuana, cocaine.
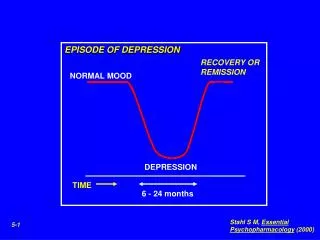
Course and prognosis • Depressive episodes vary from 4- 30 wks for mild-moderate cases, to an average of about 6 months for severe cases. • Episodes of recurrent depression tend to be shorter (4-16 wks). • 10-20% of patients will have a chronic course, with persistent symptoms lasting over 2 yrs. • The majority of patients experiencing a depressive episode will have further episodes later in life (risk of recurrence is -30% at 10 yrs, -60% at 20 yrs) • Modern antidepressant treatments impact significantly upon these figures, reducing the length of depressive episodes. Mortality • Suicide rates for severe depressive episodes vary, but may be up to 13% (i.e. up to 20 times more likely than the general population). • The overall death rate for patients with depression is higher than the general population. Cause of death is usually due to suicide, drug and alcohol problems, cardiovascular disease, respiratory infections, and thyroid disorders.
Treatment: • NICE guidelines: A number of treatments are available for depression. The two main approaches are talking (psychological) therapies, such as counselling, and treatment with antidepressant medicines. • Medication: • Antidepressants • SSRIs (selective serotonin re-uptake inhibitors) such as fluoxetine (Prozac) and paroxetine (Seroxat). • TricyclicsDosulepin (Prothiaden) and clomipramine (Anafranil) • MAOIs (monoamine oxidase inhibitors) such as phenelzine (Nardil) • Complementary therapies (a.k.a. herbal treatment) • Talking therapies: Counselling in form of a one-to-one session. • Electroconvulsive therapy (ECT)
DEPRESSION UK: • “Depression UK” (D-UK), is a national self help organisation, which was founded in 1973. It was first registered as a charity in 1979. • It has hundreds of members who either suffer from depression or have suffered from it in the past, or who care about such people. Their anonymity is strictly preserved. • Those who suffer from depression find it helpful to share their problems with fellow sufferers, because they understand the sadness, torment, and despair that this illness causes. That is why Depression UK was formed years ago to enable members to communicate with each other.The charity is run by a team of 15 or more unpaid and non-health professionals, who work mainly from their own homes. Depression UK is entirely self-funding, has no commercial links, employs no staff, and has no office headquarters. • An annual subscription of only £10 is required, or less for those who recieve benefits/ have a low income.
Their mission: • to offer fellowship to anyone troubled by depression, whoever they are. • to overcome the isolation felt by many people with depression, and to help break down the stigma attached to the illness. • to work alongside the medical and caring professions, and to attempt to meet the needs of sufferers not covered by health professionals • NOT to give medical advice or prescribe any medical treatment or product — because they are not qualified to do so.
THE DEPRESSION UK NEWSLETTER • Depression UK issues a £1.50 newsletter four or more times a year, at no extra charge to their members. This publishes members’ letters, which offer their views and ideas as to how they cope with their depression and their treatment. • http://www.depressionuk.org/join.htmlA typical newsletter also contains: • short articles • literature reviews • poetry • humorous stories, and jokes. (It does us good to laugh sometimes!) • information about depression self help groups • mention of Depression UK meetings, and the latest news.
References • Thomas CN and Morris S. Cost of depression among adults in England in 2000. Br J Psychiatry 2003;183:514-9 • NPC. Non-drug therapies for depression in primary care. MeReC Bulletin Vol.16 No.1 • Oxford Handbook of Psychiatry, 1st Edition, pg 242. • Brown GW and Harris TO (1978) Social origins of depression: a study of psychiatric disorders in women. Tavistock Publications, London. • http://www.who.int/mental_health/en/ • http://www2.netdoctor.co.uk/diseases/depression/index.asp • http://www.nhs.uk/Pathways/depression/Pages/Avoiding.aspx • http://www.depressionuk.org/ • http://www.depressionalliance.org • http://www.guardian.co.uk • http://www.overcomedepression.co.uk/ • http://www2.btcv.org.uk/display/greengym • http://www.netdoctor.co.uk/diseases/depression/drugsanddepression_000487.html • http://www.healthcentral.com/depression/treatment-000008_10-145.html • http://www.fda.gov/bbs/topics/NEWS/2006/NEW01326.html. • http://www.bupa.co.uk/