Download
1 / 55
710 likes | 2.16k Views
VENTRICULAR SEPTAL DEFECT. Dolly mathew. Development of IVS. Muscular septum – primordial IV septum Closure of interventricular foramen& membranous septum formation- Rt & Lt bulbar ridges endocardial cushions. Anatomy. A VSD is a defect in the ventricular septum

E N D
VENTRICULAR SEPTAL DEFECT Dolly mathew
Development of IVS • Muscular septum – primordial IV septum • Closure of interventricular foramen& membranous septum formation- Rt & Lt bulbar ridges endocardial cushions
A VSDis a defect in the ventricular septum • The ventricular septum consists of an inferior muscular and superior membranous portion • The membranous portion -most commonly affected in adults and older children • most common congenital cardiac anomalies. • 3-3.8 per 1000 live births • 30-60% of all newborns with a CHD • Prospective studies give a prevalence of 2-5 per 100 births of trabecular VSDs that closes shortly after birth in 80-90% of the cases
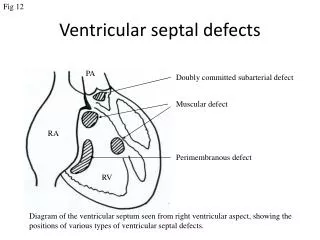
Location of VSDs outlet • perimembranous Muscular Swiss cheese Inlet
soto et al • Perimembranous(membranous/ • infracristal )-70-80% • Muscular- 5-20% Central- mid muscular Apical Marginal- along RV septal junction Swiss cheese septum – multiple defects • Inlet/ AV canal type-5-8% • Supracrital/ subaortic- 5-7%
Types of VSD (kirklin) 1 2 3 4
Hemodynamic classification • Restrictive- resistance that limits the shunt at the site of vsd LVSP > RVSP pulm /aortic systolic pressure ratio < 0.3 Qp / Qs<1.4/1 • Moderately restrictive - RVSP high, but less than LVSP - Qp/Qs 1.4/2.2 • Non restrictive -Shunt not limited at the site of defect RVSP , LVSP, PA , Aortic systolic pressures equal Qp/Qs >2.2 Flow determined by PVR
Small VSD in infancy • <1/3rd size of aortic root • shunt limited by size of the defect • Shunt entirely during ventricular systole • L R shunt <50% LV output • Pulmonary:systemic flow ratio < 2:1
Medium sized VSD • VSD size about half – equal to the size of the aortic orifice • When PA & RVSP are > 50% of systemic arterial pressure • mod-large L R shunt develops • p218
Large VSD • Size equal to the aortic root • Equalization of pressures in RV& LV • Increased LA pressure opening of foramen ovale
During systole, blood is shunted from LV to RV • passes through the lungs and re enters the LV via the pulmonary veins and LA • causes volume overload on the LV • Shunt into the RV elevates RV pressure and volume, leading to pulmonary hypertension. • More noticeable in patients with larger defects
pathophysiology • Magnitude of shunt: size, PVR • Small defect: large resistance occurs at the defect • Larger defect: resistance offered by the defect minimum : Shunt depends largely on PVR • Lower the PVR, greater the LR Shunt
Enlargement of LA, LV,PA • Shunt mainly in systole, when the RV also contracts • Shunted blood goes directly to PA
Natural history • Spontaneous closure :75-85 % all VSDs • :35% perimemb ( 1st 6/12) • More frequent in small defects • Decrease in size with age • Inlet & outlet defects donot become smaller /close spont • Large & nonrestrictive defects : 10- 15% • endocarditis– risk of endocarditis 4-10% for the first 30 years of life • High velocity turbulent jet into RV
CHF • Large VSDs • Mod sized VSDs survive into adulthood • Increased rt sided flow pulmonary vascular disease Eisenmenger’s physiology if left untreated
Risk factors for decreased survival • Shortness of breath, fatigue, DOE,progressive AR • Cardiomegaly • PASP >60mm Hg/ >1/2 of systemic pressure • Good prognosticators Lack of symptoms normal LV size & function small LR shunt normal pulmonary pressures / resistance Intact vasodilator response in pulmonary vasculature
genetic factors • Affected father- 2% • Affected mother – 6% • 25 yr survival for all pts with a VSD 87% • Mortality increases with the size of VSD
Mechanisms of closure • Growth & hypertrophy of septum around the defect • By development of subacute bacterial endocarditis • adherence of STL tissue to the margins • (Negative pressure effect exerted by a high velocity stream flowing through the defect ) • Ventricular septal aneurysm • prolapse of aortic cusp • intrusion of a sinus of valsalva aneurysm
History • Incidence unrelated to maternal age, sex, birth order • 3.3% 1st degree relatives of index patients • Among 1st degree relatives with CHD, 1/3rd have vsd • 30-60% siblings of index patients have vsd • Parents with spontaneously closed vsd can have offspring with vsd
Small VSD - infancy • Normal wt gain & development • 2-8 wks – tachycardia & tachypnea especially with infection • 2-4/6 systolic mr, medium frequency
Large VSD - infancy • Infant well in the immediate postnatal period • Systolic mr LLSB after 1-7 days • develop respiratory distress , in 2-8 wks • Cardiomegaly • Systolic thrill , along LSB • S1 normal/ soft: s2loud narrow split • Systolic mr , 2-3/6 intensity at birth, louder & harsh as shunt increases • S3 & MDM at apex • If the infant survives - subsequent course with persistent dyspnea, sweating, poor feeding, failure to thrive, LRTI
Beyond infancy • Arterial pulse- brisk ( vigorous ejection from a volume overloaded ventricle) • N pulse in eisenmenger’s - systemic stroke volume maintained • Cyanosis & clubbing : eisenmenger’s • JVP – N in small defects elevated - Mod restr & nonrestrictive vsd with ccf • Precordial bulge ( large shunt 5-6 months) • Harrison’s sulcus
Cardiomegaly • RV heave in pts with RV vol overload • Features of PAH • Grade 2-5/6 systolic regurgitantmrLLSB • MDM preceeded by S3 • Infundibularvsd: early diastolic decrescendo mr of AR
Improvement of symptoms • Closing defect findings : soft s2 high frequency & shorter murmur • Increasing PVR findings : increased RV pulsations s2 loud, narrow split • Infundibular hypertrophy decreased LR shunt, findings : s2 decreases in intensity , crescendo-decrescendo systolic murmur in the ULSB, cyanosis (shunt reversal )
Eisenmenger’s • apex by RV • Palpable dilated hypertensive pulmonary trunk • Loud pulmonary closure sound • Very short or no systolic mr of vsd • Short pulmonary ejection mr ULSB • EDM of pulmonary regurgitation • Loud harsh s1 coincident holosystolicmr of TR
ECG • small defects unremarkable • LA enlargement - Mod restrictive, large LR shunts • left axis deviation Inlet vsd /AV septal defect 5% moderately restrictive vsds Ventricular septal aneurysms multiple vsds
LV enlargement in larger defects • RVH - Mild or moderate elevation of RV pressure (rsR’ in V4R or V1) - Large VSD, equal ventricular pressures , elevated PVR • RVH , RAD - Eisenmenger’s • RBBB - Surgical repair
Chest x ray • Small defects that were mod restrictive at birth – increased LV size, dilated pulmonary trunk & its branches • Large shunts – hyperinflated lungs with flat hemi diaphragms • LA enlargement best appreciated in the lateral position • Increased PVR, decreases LR shunt, decreases heart size, enlargement of pulmonary trunk& its branches persists • Nonrestrictive vsd with elevated but variable PVR- enlargement of all 4 chambers • Eisenmenger’s syndrome- oligemic lung fields, RA,LA, LV normal, RV occupies the apex
Echocardiography- doppler • CFM-Direction, timing of flow • IVG (mmHg) = 4v² • PG = LVSP - RVSP • LVSP - PG jet = RVsp ≈ Pasp • RVSP = cuff systolic BP – 4v² • PVR = TRV / TVI in RVOT x 10 + 0.16 • High PA pressure, TRV/TVI rvot < 0.2 ; indicates low PVR, elevated pressure secondary to the flow
Cardiac catheterization Hemodynamic assessments cardiac index oximetry quantification of shunt To assess pulmonary vascular resistance • Pts with increased PVR, with mod or large LR shunt • If PVR is increased, response to 100% oxygen,NO tested
cineangiography • Defect best imaged in LAO(70°)cranial (25°) • Inlet defect - hepatoclavicular view ( 40°LAO,cranial angulation) • Anterior muscular VSD- RAO view • Aortography - r/o PDA ,coarctation
Other imaging modalities • Cardiac CT- assess VSD anatomy in suboptimal echo imges No information about shunt fraction • MRI • delineate vsd location& shunt fraction in complex associated lesions
Observation & follow up Small VSDs • Medical management Medium sized vsd CCF- treat with diuretics & digitalis, ACEI failure ppted by LRTI- Treat both 2-3 months follow up RV & PA pressures assessed Failure to thrive • Surgical Large vsd
drugs digoxin 10-20mcg/kg per day furosemide 1–3 mg/kg per day captopril0.5–2 mg/kg per day enalapril 0.1mg/kg per day
Indications of surgical intervention • Large VSD with pulmonary hypertension • VSD with aortic regurgitation • VSD with associated defects • Failure of congestive cardiac failure to respond to medications
Timing of surgery in VSD • <3months - if symptomatic • 3-6 months - symptomatic, growth failure, increasing PAH • >6 months – primarily based on PAH • Wait till 1 yr , if no PAH
Surgical VSD closure • Surgeons with training & expertise should perform VSD closure surgeries • Closure of vsd indicated when Qp/Qs 2 or more & clinical e/o LV volume overload When pt has a history of IE
IIa IIa IIa IIa IIa IIa IIa IIa IIb IIb IIb IIb IIb IIb IIb IIb III III III III III III III III I I I I I I IIa IIa IIa IIa IIa IIa IIa IIa IIb IIb IIb IIb IIb IIb IIb IIb III III III III III III III III I I I I I I IIa IIa IIa IIa IIa IIa IIa IIa IIb IIb IIb IIb IIb IIb IIb IIb III III III III III III III III I I I I I I B B IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I Surgical VSD closure • Closure of vsd is reasonable when LR shunt is present at a Qp/Qs >1.5, with a PA pressure <2/3rd of systemic pressure & pulse volume recording < 2/3rd of SVR • Closure of vsd is reasonable when LR shunt is present at a Qp/Qs >1.5, in the presence of LV systolic or diastolic failure • Vsd closure not recommended in pts with severe irreversible PAH
Interventional Catheterization for VSD • Device closure of a muscular vsd may be considered,especially if its remote from tricuspid valve & aorta, if the vsd is associated with severe Lt sided chamber enlargement, or if PAH
VSD closure • Direct closure of the defect • Surgical mortality <1% • Complications – RBBB- direct injury to rt bundle, disruption of purkinje fibers • Residual shunt (<5% ) • Injuries to tricuspid valve & aortic valve
PA banding • PA banding- palliative procedure , when additional lesions make repair difficult • Done in multiple VSDs • 30-50% of original diameter is narrowed • Systolic pressure of 25-30 mmHg beyond the constriction • RV/PA pressure gradient > 45 associated with hypoxemia