Download
1 / 66
680 likes | 1.1k Views
Week 8c Chapter 36 Early Effects of Radiation. In the 1920’s & 1930’s if was not uncommon for radiologic technologist to get hematologic exams weekly. Blood work was used to monitor the worker for over exposure before dosimeters were available.

E N D
Week 8c Chapter 36 Early Effects of Radiation • In the 1920’s & 1930’s if was not uncommon for radiologic technologist to get hematologic exams weekly. • Blood work was used to monitor the worker for over exposure before dosimeters were available. • In the 1960’s blood work was done quarterly and dosimeters were worn.
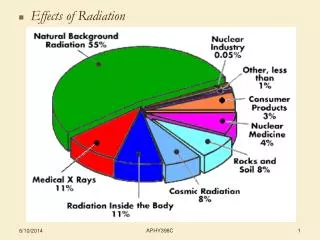
Early Effects of Radiation • In humans, a response to radiation that occurs within months of the exposure is called Early Effects. • Death is the most devastating human response to radiation. No deaths immediately after diagnostic radiography have ever been reported.
Early Effects of Radiation • Many of the pioneers in radiology died from long term effects of exposure. • Diagnostic x-ray beams always result in partial body exposure, which is much less effective at producing a response than whole body exposure.
Major Lethal Exposures in Humans • 1945 Atomic Bombs in WW2 • 1979 Three Mile Island Nuclear Power Plant Accident killed one person. • 1986 Chernobyl Russia nuclear reactor melt down killed 30 people (official) 500,000 reported. • Military accidents have also killed humans.
Acute Radiation Syndrome • 1. Prodormal period: acute symptoms within hours of exposure. • 2. Latent period: time free of any visible effects. • 3. Manifest illness: • Hematologic syndrome • Gastrointestinal syndrome • Central Nervous System Syndrome • 4. Recovery or Death
Prodromal Period • Prodromal period may last for a few hours or a couple of days. • Symptoms include nausea, vomiting and diarrhea. • Severity of symptoms are dose related. • For extremely high exposure it is hard to distinguish Prodromal from manifest illness
Latent Period • After prodormal radiation sickness there is a period of apparent well-being called the Latent Period. • With very high exposure, it may last only a few hours. For lower exposures, it may last for weeks. • May be mistakenly thought to be recovery from moderate exposure.
Latent Period • Biologic and physiologic changes are occurring even though they give no indication of the response yet to follow. • Responses are extremely variable relative to dose. • High exposure will skip the latent period while low exposure may not have the Prodromal period.
Manifest Illness • Manifest Illness is a dose related period characterized by three separate syndromes. • Hematologic Syndrome • Gastrointestinal Syndrome • Central Nervous System Syndrome
Hematologic Syndrome • The hematologic syndrome is produced with exposures of 200 to 1000 rads. • The prodormal period will be rather mild lasting for a few hours to a couple of days. The latent period may last for a month.
Hematologic Syndrome • There are no obvious signs of illness, although the number of cells in the peripheral blood is declining. • Manifest illness is characterized by vomiting, mild diarrhea, malaise, lethargy and fever. All types of blood cells are depleted.
Hematologic Syndrome • If the patient recovers, recovery will begin in two to four weeks. • If the exposure is severe, the cell depletion will continue until the body no longer has any defense from infection. • Just before death, infections and dehydration will be pronounced.
Gastrointestinal Syndrome • After radiation exposures of 1000 to 5000 rads, the GI syndrome occurs. • The Prodromal symptoms of vomiting and diarrhea occur within hours and may last for days. • A latent period of 3 to 5 days follows with no apparent symptoms.
Gastrointestinal Syndrome • The manifest illness phase begins with a second wave of nausea and vomiting followed by diarrhea. • Patient my loose appetite and become lethargic. Diarrhea increases to watery and then bloody stools. • Death occur occurs in 4 to 10 days.
Gastrointestinal Syndrome • Intestinal cells are normally rapidly proliferating. Radiation kills the stem cells stopping repopulation. • At the level of exposure for GI syndrome, hematologic damage also occurs but the response is slower so the patient dies before the manifest symptoms occur.
Central Nervous System Syndrome • CNS Syndrome occurs with exposures greater than 5000 rads. • A series of signs and symptoms occur that leads to death in a matter of hours to 3 days. • First is nausea and vomiting minutes after exposure
Central Nervous System Syndrome • Within the first hour. • The person will become extremely nervous and confused. • Complain of burning sensation in the skin. • Loss of vision and consciousness. • A latent period of about 12 hours follows with the symptoms subsiding.
Central Nervous System Syndrome • Manifest illness begins with the prodromal signs returning with increased intensity. • Person becomes: • Disoriented; • Looses muscle coordination • Difficulty breathing
Central Nervous System Syndrome • Person experiences: • Loss of equilibrium • Convulsive seizures • Ataxia • Lethargy • Coma followed by death. • The ultimate cause of death is increased fluid content of the brain.
LD50/60 • The LD50/60 is the dose of whole body radiation necessary to kill 50% of the population in 60 days. • For humans the lethal dose is 350 rads. With medical support, humans can survive 850 rads.
Local Tissue Irradiation • When only a localized area is irradiated, higher dose is required to produce a response. • Every organ and part of the body can be affected by partial body irradiation. The affects of cell death is shrinkage or reduction in size of the tissue or organ. This is called atrophy.
Local Tissue Irradiation • If the dose is high enough, any tissue will have immediate response. • Tissue types that are commonly affected immediately are: • Skin • Gonads • Bone Marrow
Effects on Skin • The skin is the tissue that we have the most experience. • Normal skin consists of three layers: • An outer layer (epidermis) • An intermediate layer of connective tissue (dermis) • A subcutaneous layer of fat and connective tissue.
Effects on Skin • Additional accessory structures of the skin include: • Hair follicles • Sweat glands • Sensory Receptors • All skin layers and accessory structures participate in the response to irradiation.
Effects on Skin • Like intestinal cells, skin cells have a continuous cell renewal but at a much slower rate. • The epidermis consists of several layers of cells with the inner most being basal cells. • Basal cells are stem cells that as the mature migrate to the surface.
Effects on Skin • One of the common responses of the skin during radiation therapy is a Erythema or a sun burn like reddening of the skin followed in a couple of weeks by desquamation or ulceration and denudation of the skin.
Skin Reaction to High Exposure • These are serial photographs on a patient that had multiple long fluoroscopic examination. • Last image is after skin graphs.
Effects on Skin • Many of the pioneers of radiography including Roentgen suffered from radiation induced skin burns. • Patients were exposed for up to 30 minute exposures so burns were common • Low level exposures do not cause Erythema.
Effects on Skin • Intermediate exposures depend upon the individual’s radiosensitivity, the dose rate and the size of the area of exposure. • High exposure will cause a response for all people. • The Skin Erythema Dose 50 would be a dose causing Erythema half the time.
Effects on Skin • Another skin response is hair loss or epilation. • For many years soft rays (10 to 20 kVp) called Genz rays were used to treat many skin diseases such as ring worms. • Tinea Capitis or ring worm in the scalp was successfully treated with Genz rays. • Often the hair would fall out for months.
Effects on Skin • Today the exposure of the skin is currently receiving more close attention because of high dose fluoroscopy. • During interventional fluoroscopy, the patient may receive 20 R/ minute so hazards do exist.
Effects on Gonads • Human gonads are critically important target organs because they are particularly sensitive to radiation. • Responses to exposures as low as 10 rads have been observed. • Since these organs produce germ cells that control fertility and heredity, their response is well studied.
Effects on Gonads • Cells from the testes and ovaries respond to radiation differently due to differences in the progression from stem cells to mature cells. • Germ cells are produced by both ovaries and testes but they develop at different rates and at different times.
Effects on Female Gonads • During the late fetal life, many primordial follicles grow to encapsulate the oogonia, which become oocytes. • These follicles remain suspended state of growth until puberty.
Effects on Female Gonads • At puberty, the follicles rupture with regularity, ejecting a mature germ cell called the ovum. • There will be only about 400 to 500 such ova available for fertilization during the next 30 to 40 years. • Radiation effect on the ovaries are age dependent.
Effects on Female Gonads • During fetal life and into early childhood, the ovaries are especially radiosensitive. • They decline in sensitivity reaching a minimum between 20 and 30 years old. • After age 30, they increase in radiosensitivity with age.
Effects on Female Gonads • The most radiosensitive cell during female germ cell development is the oocyte in a mature follicle. • Doses as low as 10 rads have resulted in a delay or suppression of menses. • 200 Rads produce pronounced infertility.
Effects on Female Gonads • 500 rad will result in permanent sterility. • Doses of 25 to 50 rad are associated with measurable increases in genetic mutation.
Effects on Male Gonads • The testes like the ovaries will atrophy with high doses of radiation. • The earliest stage of cell development is the time of greatest radiosensitivity. • Therefore effects will not be apparent for 3 to 5 weeks.
Effects on Male Gonads • Exposures of 10 rad have resulted in a reduction of sperm. • 200 rad will produce temporary sterility. • 500 rad produces permanent sterility.
Effects on Male Gonads • After an exposure of 10 rad, the male patient should refrain from procreation for two to four months so the irradiated cells have matured and disappeared. • There will still be a possibility of genetic damage.
Hematologic Effects • The Hemopoietic System consists of: • Bone Marrow • Circulation Blood • Lymphoid Tissue • Lymph Nodes • Spleen • Thymus
Hematologic Effects • All tissue develop from the same stem cell called a pluripotential stem cell. • Although the spleen and thymus produce one type of leukocyte, the lymphocyte, most circulating lymphocytes are produced in the bone marrow.
Hematologic Effects • In children, bone marrow is rather evenly distributed through out the skeleton. • In adults, the active bone marrow is limited to the flat bones and the ends of long bones.
Hematologic Effects • From a single pluripotential stem cell, a number of cells are produced. • Lymphocytes used in the immune response. • Granulocytes scavenger cells used to fight bacteria. • Thrombocytes or Platelets • Erythrocytes Red blood cells that carry oxygen.
Hematologic Effects • The principle response to irradiation is a depletion of all types of blood cells. Lethal exposure to the stem cells and other precursor cells cause the depletion. • Lymphocytes are the first cells to be affected. Almost immediately the numbers are reduced directly by the exposure.