Download
1 / 31
330 likes | 1.11k Views
The face in diffuse Systemic Sclerosis: note the radial furrows surrounding the mouth, pinched nose and scattered telangectasia. This patient had a 20 year history of Raynaud's phenomenon and hand stiffness. In the last few years she noticed the appearance of several

E N D
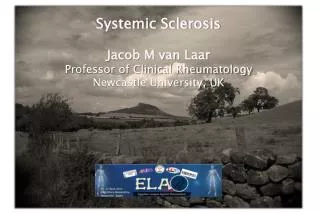
The face in diffuse Systemic Sclerosis: note the radial furrows surrounding the mouth, pinched nose and scattered telangectasia.
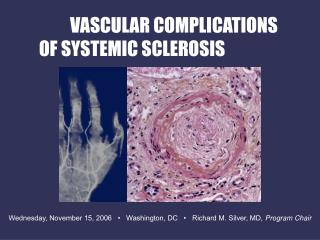
This patient had a 20 year history of Raynaud's phenomenon and hand stiffness. In the last few years she noticed the appearance of several telangectasia on the skin and started suffering from dysphagia and heartburn. For one year before coming to our Department she had been treated with nifedipine 20mg/d. Physical examination revealed : - sclerodactyly and pitted scars on the finger-tips, - widespread telangectasia involving the face, upper trunk and extremities, - microstomia with angular creases, - radial furrows - mild hypertension. Case 1a:Clinical Background
EGDS showed severe esophagitis, distal esophageal dilation and hiatus hernia. Esophageal manometry showed decreased amplitude and incoordination of peristaltic waves in the distal esophagus and inadequate lower esophageal sphincter competence. In addition 24-hour pH monitoring showed an abnormal acid exposure of the distal esophagus and decreased clearing ability. Chest radiograph and pulmonary function tests (including carbon monoxide diffusing capacity) were normal. She had no electrocardiographic or echocardiographic evidence of cardiac involvement. Urinalysis and other indicators of renal function were within normal limits. She was discharged on penicillamine (150 mg/d), nifedipine (20 md/bid) and gastric antacids. Case 1b:Clinical Background
Radial furrows: initial manifestations in a 38 year old woman with diffuse Systemic Sclerosis.
Indurative phase: the skin is shiny, taut and tightly adherent to the underlying structures
The "neck sign" with beading, ridging, and hypopigmentation.
Case 2 : Clinical background A 42 year old woman with a one-year history of Raynaud's phenomenon. Previous extensive investigations were not significant: the patient had anti-Scl-70 antibodies and an initial scleroderma pattern on capillaroscopy but no evidence of visceral or cutaneous involvement. One month before coming to our Department (while being treated with nifedipine 10mg bid alone) she noticed the appearance of a slightly indurated plaque on both sides of the neck. Physical examination revealed two 4-5 cm in diameter superficial yellow-brown plaques extending to the lateral sides of the neck and the supraclavear area. The skin appeared thickened but still somewhat elastic and the surface was smooth but irregular due to a network of closely packed broad based papules (beading). There was no sclerodactyly, pitted scars, telangectases or other cutaneous evidence of systemic sclerosis. She was treated with griseofulvin (500 mg/d) for 9 months with initial improvement. However, during the following months, she started complaining of hand stiffness and developed slight sclerodactyly. Penicillamine treatment was therefore started.
Raynaud's phenomenon: white areas due to vasoconstriction.
Hand involvement in diffuse systemic sclerosis: - note flexion contractures of the fingers, - shortening of the terminal phalanges as a result of distal bone resorption, - and nail dystrophy.
Case 3:Clinical Background • A 36 year old male patient who, at the age of 30 yrs, noticed Raynaud's phenomenon and progressive stiffness and tightness involving the skin of the hands and face. • He received no medical treatment for 6 years and when he was finally admitted to our Department he had advanced acrosclerosis and a severe pulmonary involvement. • Antinuclear autoantibodies on HEp-2 cells and anti-Scl-70 were found.
Hand involvement: note dystrophic scarring of the fingertips.
Case 4 :Clinical Background A 38 year old male patient. Onset at the age of 34 years with stiffness and Raynaud's phenomenon soon followed by swelling of the fingers due to soft tissue edema and a symmetric polyarthritis involving the hands, wrists, elbows, ankles and knees. For two years he received NSAIDs alone with significant improvement in the articular symptoms.Because of the progression of hand involvement he was referred to our Department. Physical examination revealed sclerodactyly and dystrophic scarring of the fingertips but no typical face involvement or proximal scleroderma. Laboratory investigations showed antinuclear and anti-Scl 70 autoantibodies. Respiratory function tests were not significant while esophageal manometry demonstrated initial asymptomatic esophageal involvement with normal acid exposure on 24-hour pH-monitoring. No signs of calcinosis on the hand X-rays and a scleroderma pattern (slow) at capillaroscopy were observed. The patient was discharged on penicillamine and nifedipine.
Gangrene of the distal phalanges in a patient with severe Raynaud's phenomenon and acrosclerosis.
Ischemic ulcers of the toes in a patient with diffuse Systemic Sclerosis.
Ischemic toe in a patient with diffuse Systemic Sclerosis: note nail dystrophy.
Localized morphea (1)Different stages of the clinical evolution Bright red erythema surrounding a central area of indurated skin with a yellow-brown color and a smooth surface.
Localized morphea (2)Different stages of the clinical evolution Long-standing plaques of morphea.Both plaques have an erythematous halo (lilac-ring) and a sclerotic ivory-white central areas with a mottled brown hyperpigmentation.
Localized morphea (3)Different stages of the clinical evolution Sclerotic, ivory-white, shiny plaque on the back.
Localized morphea (4)Different stages of the clinical evolution Active plaque of morphea with an erythematous halo (lilac-ring) and a thickened, sclerotic, yellowish area in the center.
Localized morphea (5)Different stages of the clinical evolution Irregular sclerotic plaque of morphea on the popliteal fold extending upwards.
Dermatology Image Atlas - Johns Hopkins University dermatlas.med.jhmi.edu/derm/
Case Generalized fibrotic bound down skin with sclerodactyly and hypopigmentation This 8-year-old girl developed progressive systemic sclerosis with sclerodactyly.
Tight fibrotic atrophic skin with narrowing of the fingers and patchy depigmentation This 28-year-old woman had progressive systemic sclerosis with Raynaud phenomenon and sclerodactyly.
Necrotic purple papules with black crusts and ulcers This 20-year-old man complained of shortness of breath. Evaluation revealed a history of Raynaud syndrome, digital infarcts, and other findings typical of scleroderma.
Extensive 1-4 mm telangiectasias This 39 year old woman with Raynaud's syndrome and scleroderma demonstrates extensive telangiectasias on her fingers. She also had widespread telangiectasias on her face, trunk and extremities.
Telangiectasias on palms A 52 year old woman with the CRESTsyndrome variant of scleroderma developed diffuse progressivetelangiectasias which were most prominent on her hands.
Telangiectasias on palms A 52 year old woman with the CREST syndrome variant of scleroderma developed diffuse progressive telangiectasias which were most prominent on her hands.
A 34 year old woman with CREST syndrome developed widepsread telangiectasias on her face, trunk and extremities.