Download
1 / 60
850 likes | 2.49k Views
Multiple Sclerosis (MS). Dr Oliver Lily Consultant Neurologist Leeds General Infirmary. Multiple sclerosis. What is MS? What causes MS? Symptoms and signs of MS Making the diagnosis Investigations Treatments. Case Study: Ms A. 20 year old medical student

E N D
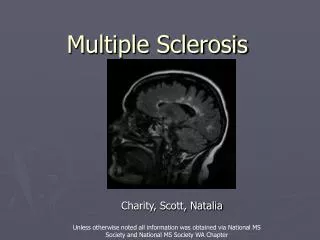
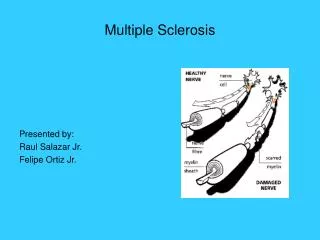
Multiple Sclerosis (MS) Dr Oliver Lily Consultant Neurologist Leeds General Infirmary
Multiple sclerosis • What is MS? • What causes MS? • Symptoms and signs of MS • Making the diagnosis • Investigations • Treatments
Case Study: Ms A • 20 year old medical student • Presented with 3 day history of pain in the left eye with blurred vision • On examination: • Reduced colour vision (Ishihara chart) • Reduced pupillary light responses (RAPD) • Hole in visual field (scotoma)
Case Study: Ms A • Next day, awoke to find vision completely gone in left eye! • Diagnosis?
Optic Neuritis • Inflammation of the optic nerve • Causes pain and loss of vision • Frequently not visible (retrobulbar) • Good prognosis: 95% return to visual acuity of 6/12 or greater within 12 months • High dose steroids speed up rate of recovery but have no effect on final acuity • 50% go on to develop MS within 10 years
Case Study: Ms A • Eye completely better within 3 months with no treatment. • Well for 2 years • Week of medical finals, complained of tingly numbness starting in both feet and gradually ascending to level around chest “like a tight band”. Felt unsteady walking and fatigued easily. • Electric shock sensations running down body whenever she bent her head • What is the diagnosis now?
Transverse myelitis • Inflammation inside the spinal chord • Often mild with good prognosis • Often pure sensory • Lhermittes phenomenon • May affect bladder • 50% go on to develop Multiple Sclerosis
Other causes of myelitis • Infective • Herpes Zoster • HTLV-1 • Lyme disease • Autoimmune • Lupus • Sjogrens syndrome • Neuromyelitis optica • Long spinal lesion (3 segments) • Anti-aquaporin antibodies
Diagnosing MS • Clinical diagnosis • Relies on dissemination in time and place • ? Is this MS
Clinically Definite MS Optic neuritis and transverse myelitis at different times Not definite MS Clinically isolated syndrome (CIS) Myelitis and optic neuritis at the same time Recurrent myelitis Recurrent or sequential optic neuritis Diagnosing MS
What is MS? • MS is the most common cause of neurological disability in young adults in the UK • 792 people with MS in Leeds • 40 new cases of MS / year
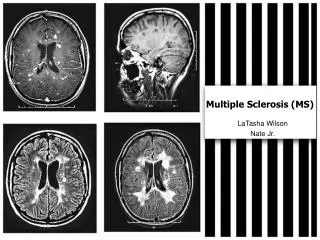
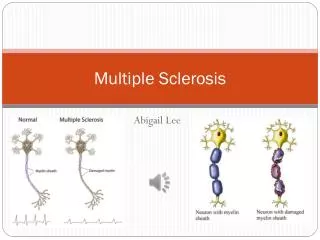
What is MS? • MS is a disease of the central nervous system (CNS) • An inflammatory reaction in the CNS causes loss of myelin and slowing of nerve conduction • Areas of demyelination • Loss of axons
Outcome: Ms A • Treated with intravenous methylprednisolone 1g daily for 3 days • Improved to normal over next 6 weeks • Told she had diagnosis of relapsing-remitting multiple sclerosis • Started on treatment with beta-interferon 1a injections • Remained in remission for next five years
Disease modifying treatments:Immunomodulation • Interferon beta 1-b • Interferon beta 1-a • Glatiramer acetate / Copaxone
Interferon beta • Reduces the number of relapses by 30% compared to placebo • Effective early in the disease course • No evidence on long-term effect on disability
The case of Dr A • Now working as a GP • 34 years old • Noticing that when she walks, after a mile or so her left leg tingles and begins to drag. If she stops for a few minutes she can carry on normally. • Referred for physiotherapy • Returns two years later. Is limping on left leg and carries a walking stick. Right leg also feels stiff and wooden. Noticed urinary urgency and occasional spasms in the legs
Case of Dr A • On examination has weakness of flexors more than extensors worse on the left, with a left sided foot drop. There is increased tone and sustained clonus in both legs with very brisk reflexes and upgoing plantars. • Spastic paraparesis – suggests a spinal chord problem • ? diagnosis
Axonal loss in MS Disability Time
Axonal loss in MS Disability Axonal loss Inflammation Time
The case of Dr A • Over the next five years walking becomes more difficult and she has to start using two elbow crutches and then a wheelchair • Her interferon is stopped but she continues with regular physiotherapy • She gets more forgetful, and eventually retires from the health service aged 42 • 15% of MS patients are confined to a wheelchair within 10 years of diagnosis
Newer treatments for RRMS:the return of immunosuppression! • Mitoxantrone • Natalizumab • Oral Treatments (Fingolimod)
Edan G, et al.Therapeutic effect of mitoxantrone combined with methylprednisolone in multiple sclerosis: a randomised multicentre study of active disease using MRI and clinical criteria. (n=42) Journal of Neurology, Neurosurgery and Psychiatry 1997;62:112-118.
Edan G, et al.Therapeutic effect of mitoxantrone combined with methylprednisolone in multiple sclerosis: a randomised multicentre study of active disease using MRI and clinical criteria. (n=42) Journal of Neurology, Neurosurgery and Psychiatry 1997;62:112-118. Hartung H-P, et al.Mitoxantrone in progressive multiple sclerosis: a placebo controlled, double-blind, randomised, multicentre trial.(n=194) Lancet 2002;360:2018-2025.
Mitoxantrone • Rapidly progressive patients • Improvements in disability/mobility as well as relapse rates (up to 90%) • Prolonged improvement (up to 18m after treatment) • 1 in 300 chance of secondary leukaemia • Dose related cardiomyopathy
Mitoxantrone chemotherapy 35 responders 30 failures 25 20 Diseaseduration 15 10 5 0
Natalizumab (Tysabri) VCAM-1 = vascular cell adhesion molecule-1.Lobb RR et al. J Clin Invest. 1994;94:1722-1728.
1. Connell B et al. Ann Neurol. 1995;37:424-435. 2. von Adrian UH et al. N Engl J Med. 2003;34:68-72.
1. Cannella B et al. Ann Neurol. 1995;37:424-435. 2. von Andrian UH et al. N Engl J Med. 2003;348:68-72. 3. TYSABRI® (natalizumab) US Prescribing information, 2004.
Elan shares dive on drug setback Shares in Irish drugmaker Elan have plummeted once more after a third case of disease linked to Tysabri, its multiple sclerosis treatment. Elan suspended the drug after two patients were found to have caught the rare disease, one of whom later died. The newly revealed case - which also ended with the death of the patient - could mean Tysabri never makes it back onto the market, analysts warned. By the close of trading, Elan shares were down 56% to 2.43 euros. The initial cases had involved patients taking both Tysabri and US firm Biogen Idec's drug Avonex, and Elan had hoped that the problem was due to an unexpected problem with the combination. The latest, however, involves Tysabri alone. Biogen's shares were down 11% by 1600 GMT.
Tysabri • Rapidly evolving MS • Monthly infusions • 67% reduction in relapse rate • 95 cases PML worldwide (50 deaths) • Chance ranges from 1 in 10000 (JC seronegative 1st year) to 1 in 125 • Yearly MRI surveillance
Fingolimod (Gilenya) • Sphingosine-1-phosphate receptor blocker; traps lymphocytes in lymph nodes • Licenced for rapidly evolving MS (second line) • 60% reduction in relapse rate • Side effects include bradycardia, macula oedema, infections (esp herpes virus), skin cancers
Drugs/treatments for MS with no proven benefit over placebo • Naltrexone • Vitamin D, E, B12, fish oils • Special diets • Venous angioplasty/stenting • Stem cell treatments (other than bone marrow transplant) • Sativex
Sativex • 160 people with MS took part in this trial which compared the effects of Sativex versus placebo on spasticity, spasms, pain, bladder and tremor. No significant improvements were seen in overall symptom relief • 189 people with MS and spasticity symptoms took part in a study which compared the effects of Sativex versus placebo. Changes in spasticity during the six-week study were recorded using a patient-reported scale and a clinical measure of spasticity. Improvements were seen on the patient-reported scale but improvements seen on the clinical scale did not reach statistical significance.
Why do MS patients consult? • Relapses: Least likely reason