Download
1 / 57
570 likes | 834 Views
The Child with Endocrine Dysfunction. Hockenberry Chapter 38 ATI pg. 333-373, 408-429 Dondi Kilpatrick RN, MSN. Learning Objectives. List Signs and Symptoms Verbalize treatment plan for : Diabetes Type I and II Hyperglycemia Hypoglycemia Growth Hormone Deficiency Growth Hormone Excess

E N D
The Child with Endocrine Dysfunction Hockenberry Chapter 38 ATI pg. 333-373, 408-429 Dondi Kilpatrick RN, MSN
Learning Objectives • List Signs and Symptoms • Verbalize treatment plan for : • Diabetes Type I and II • Hyperglycemia • Hypoglycemia • Growth Hormone Deficiency • Growth Hormone Excess • Diabetes Insipidus • SIADH • Hypothyroidism • Hyperthyroidism
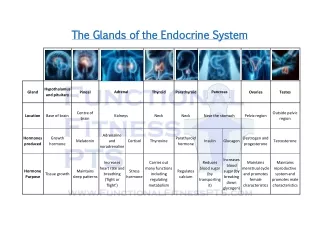
Disorders of Pancreatic Hormone Function Review • Islets of Langerhans 3 major functioning cells • Alpha cells • Beta cells • Delta cells • Balance out the insulin and glucagon
Diabetes Mellitus (DM) • Metabolic disorder • Chronic hyperglycemia • Total /partial deficiency of hormone INSULIN • Impairs the body’s ability to use food for energy • Most common chronic endocrine disorder of childhood • No cure
Diabetes Mellitus (DM) Type 1 • Beta cell destruction • Leads to absolute insulin deficiency • 5-10% of all DM cases Type 2 • Insulin resistance • 90-95% of all DM cases • Historically more common in adults > 45 • prevalence seen in children/adolescents
Causes Type 1 • 2 types • Auto immune • Idiopathic • Not simple inheritance • Genetic predisposition plus trigger event Type 2 • Insulin resistance plus relative insulin deficiency
Risk factors for Type II • Overweight • Decreased exercise pattern • Family history of type 2 DM • Age • Non-European ancestry
Signs and Symptoms Type 1 • Polyuria • Polydipsia • Polyphagia • Rapid weight loss • Dry skin • Irritability • Drowsiness/fatigue • Abdominal discomfort • Ketoacidosis Type 2 • Polyuria • Polydipsia • ↑ BP • Frequent infections • Fatigue • S/S insulin resistance • Acanthosis nigricans • Polycystic ovary disease
Acanthosis nigricans www.aocd.org/skin/dermatologic_diseases/acanthosis Acanthosis nigricans screening program
Treatment Team approach!!! • Type 1 • Insulin! • Monitor glucose levels • Lifestyle changes • Nutrition • Exercise Type 2 • Lifestyle changes • Nutrition • Exercise • Oral meds • Monitor glucose levels
Insulin • Types • Human • Most of what we see • Pork • Not used much at all • All types • 100 units/ml
Types of Insulin • Based on: • Onset • Peak • Duration • 5 types • Rapid • Short • Intermediate • Long • Mixed
Types of Insulin • Rapid • Give within 15 minutes of a meal!!! • Intermediate • Is cloudy • Long acting • Lantus can’t be mixed in a syringe with any other insulin
Insulin Mixtures • 70/30; 50/50; 75/25 • 1st # - % of intermediate insulin • 2nd # - % of short or rapid acting insulin • Pay attention to the name of the mix!!!! • 70/30 is 70% NPH and 30% short acting
Mixing Insulin • Administer mixed insulin within 5 minutes of mixing or wait 15 minutes • Ignore this slide, she won’t test us on it
Insulin Dosing • One dose a day rarely suffices • Split mix is common • Rapid/short acting mixed with NPH • Given prior to breakfast and supper • For better control- multiple injections
Insulin Administration • Subcutaneous administration • Rotate sites • Insulin absorption • Abd is fastest, arm is next, and the leg is the slowest www.rch.org.au/diabetesmanual/manual.cfm?doc_id=2733#injection_sites
Insulin Administration • Complications • Lipoatrophy • Where the tissue atrophies or breaks down, little pitting areas • Lipohypertrophy • Build up of fat, like a fatty nodule
Insulin Administration • Insulin pen • Resembles a large fountain pen • Needle is screwed onto tip immediately prior to injection
Insulin Administration • Insulin pump • Computerized device • About the size of a pager • Worn around the waist • As close to normal insulin delivery as possible now • Drawbacks • Pump malfunction, can’t get air in line, have to know how to do calculations and work the device
Insulin Administration • Absorption can be altered • exercise • illness • Self monitoring is a must!!! • This disease is lifelong so when the kid gets old enough to do the shit himself, he needs to do the shit himself
Oral Medications • Type 2 DM children only • Used if lifestyle changes are not effective • Decreases absorption of blood sugar from the diet, reduces the insulin usage.
Monitoring • Self- blood glucose monitoring • At home & in hospital • Goal- blood glucose 80-120 mg/dl • Glycosylated hemoglobin (Hgb A1c) • Typically levels of 6.5%-8% are acceptable • Blood sugar attaches to the hemoglobin for the life of the hemoglobin, the hemo lives about 120 days • A level of 6% means your avg blood sugar is about 120 • Every number increase is about an increase of 30. So 7% is about 150
Monitoring • Finger sticks / Atraumatic care • Warm the finger • Use the ring finger and thumb • They bleed a little bit easier • Puncture to the side of the finger pad
Complications Hyperglycemia • Caused by: • Too little insulin • Illness/infection • Injury • Stress- physical/emotional • Decreased exercise • Diet
Hyperglycemia • Symptoms • 3 P’s • Nausea • Blurred vision • Fatigue • Diabetic ketoacidosis (DKA) • Treatment • Drink extra fluids • Administer additional insulin • Monitor glucose more closely
Complications- Hypoglycemia • Caused by: • Too much insulin • Diet • Exercise • Growth spurts • Puberty • Illness/injury • Menses
Hypoglycemia Symptoms • Mild-moderate • Shaky/sweaty • Hungry • Pale • Headache • Confusion • Disorientation • Lethargy • Change in behavior • Severe • Inability to swallow • Seizure/convulsion • Unconsciousness
Hypoglycemia • Treatment • Often difficult to differentiate HYPO from HYPERglycemia • Check blood sugar if possible • When in doubt, give simple carbohydrate • Follow with complex carbohydrate, then protein
Hypoglycemia • If unconscious, seizes or cannot swallow • Glucagon • Mixed and given IM/SQ • Releases stored glycogen from liver • Should increase blood glucose in 15 minutes • Can cause nausea/vomiting • Protect from aspiration
Somogyi Effect • Hypoglycemia followed by rebound hyperglycemia • More common for type I, especially in children • Signs and symptoms • Treatment – reduce bedtime insulin to prevent early a.m. hypoglycemia
Long Term Complications • Vascular changes • Involve large and small vessels • Heart disease • Retinopathy • Neuropathy • Arterial obstruction • Gangrene
Education • Always carry: • Glucose tablets • Insta-glucose • Sugar cubes • Candy • **children may fake a reaction to get candy** • Exercise • With good control: • Decreases insulin requirements • With poor control • May stimulate ketoacidosis
Education • Nutrition • Sufficient calories to balance daily expenditure for energy and growth • Constant carbohydrate diet-exchange system • Consistent intake/timing of food • Timing of food coincides with time/action of insulin • Total # of calories/proportions of basic nutrients needs to be consistent day to day
Type I Diabetes • Allow toddler and preschooler to make food choices - monitor Carbohydrates • Monitor temper tantrums as possible signs of hypoglycemia • Snacks should be available during increased activity such as sports activities
Estimating Portion Sizes • for eyeballing portion size: • 1 ounce of cheese is as big as 4 dice • ½ cup of rice is as big as half a baseball • A 4-ounce bagel is the size of a hockey puck • 3 ounces of meat is as big as a deck of cards • 2 tablespoons of peanut butter is about a Ping-Pong ball • 1 cup of pasta equals a tennis ball www.lillydiabetes.com
Education • Illness management • Monitor glucose every 3 hours • Monitor urine ketones every 3 hours or when glucose is > 240 mg/dl • Urine ketones are not used for daily management
Disorders of Pituitary Function • Pituitary gland • “Master” gland • Regulates other endocrine functions • Releases or withholds 7 other hormones • Growth hormone (GH)
Hypopituitarism • Caused by: • Organic lesions (tumors) • Idiopathic • Usually r/t GH deficiency
GH deficiency • Manifestations • Short stature – usually below 5th percentile • Usually grow normally 1st year • During the 2nd year growth drops off established percentile • Height may be more retarded than weight • Normal skeletal proportions • Sexual development usually delayed, but normal • Most have normal intelligence
GH deficency • Diagnosis • Physical exam • Family history • X rays • Endocrine studies • Growth chart
GH deficiency • Treatment • Correct underlying disease process • Replacement of GH (80-90% successful) • Biosynthetic GH drug of choice • FDA approved for: • GH deficiency • Chronic renal insufficiency • Prader-Willi syndrome • Turner syndrome
Growth Hormone Excess • Hyperpituitarism • Over secretion occurs prior to epiphyseal plate closure • Grow 7-8 feet tall • Acromegaly • Over secretion occurs after epiphyseal plate closure • Overgrowth of head, lips, nose, tongue, jaw, separation malocclusion of teeth, increased facial hair
Growth hormone excess • Treatment • Remove tumor, pituitary gland radiation, high dose sex steroids to close growth plates
Diabetes Insipidus (DI) • Disorder of the posterior pituitary • Results from HYPOsecretion of Antidiuretic Hormone (ADH) • ADH sometimes called vasopressin (Pitressin) • Produces uncontrolled diuresis • Causes • Primary: familial or idiopathic • Secondary: trauma, tumors, CNS infection, aneurysm
Diabetes Insipidus (DI) • Manifestations • Cardinal signs: POLYURIA & POLYDIPSIA • 1st sign is often ENURESIS • Infants: • irritability relieved with feeding of WATER not milk • dehydration often occurs
Diabetes Insipidus (DI) • Management • Instruct parents there is a difference between DI and DM • Daily hormone replacement of vasopressin • Drug of choice: DDAVP • Nasal spray or IV • Treat for lifetime
Syndrome of Inappropriate Antidiuretic Hormone (SIADH) • Disorder of posterior pituitary • Produces HYPERsecretion of ADH • ADH causes reabsoption of water back into central circulation • Causes • Infection • Tumors • Trauma • CNS disease
SIADH • Manifestations • Fluid retention but no edema • HYPOtonicity • Anorexia • Nausea/vomiting • Irritability • Personality changes
SIADH • Treatment • Fluid restriction • ¼-½ of maintenance • We don’t want further dilution in their body • Correction of underlying disorder (infection, tumor resection, etc.) • They may receive some diuretics, make sure to tell the families to get rid of other sources of water (toilet, plants, dog bowls)