Download
1 / 60
600 likes | 628 Views
Endocrine Dysfunction: Adrenal & Pituitary. Endocrine System. Endocrine System (comprehensive source) Endocrine Review (narrated online review) Medications-Endocrine (narrated PPTs) Endocrine Drugs Overview Pituitary Drugs Adrenal Drugs. Pituitary Gland - “master gland” + Hypothalamus.

E N D
Endocrine Dysfunction:Adrenal & Pituitary Endocrine System Endocrine System(comprehensive source) Endocrine Review (narrated online review) Medications-Endocrine (narrated PPTs) Endocrine Drugs Overview Pituitary Drugs Adrenal Drugs
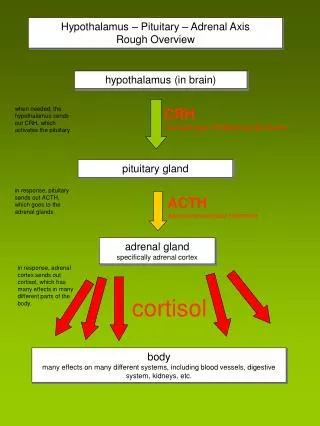
Hypothalamus-functions Hypothalamus- integrative center for endocrine and autonomic nervous system *Hypothalamus and pituitary - integrate communication between nervous and endocrine system Control of some endocrine glands by neural and hormonal pathways Two major groups of hormones secreted: inhibiting and releasing
Hypothalamus Two major groups of hormones secreted: inhibiting and releasing
ANTERIOR PITUITARY (Adenohypophysis) • SECRETES 6+ HORMONES: • ACTH (adrenocorticotropic hormone) controls release of cortisol in adrenal glands • *ACTH release; controlled by corticotropin-releasing hormone (CRH)
ANTERIOR PITUITARY(adenohypophysis) • TSH (thyroid stimulating hormone) • Thyroid –releasing hormone; secreted by hypothalamic neurons-control release of TSH • GH (growth hormone) (Somatotropin) stimulates growth of bone/tissue
Prolactin-promotes mammary gland growth and milk secretion • FSH (follicle stimulating hormone)- stimulates growth of ovarian follicles & spermatogenesis in males • LH (lutenizing hormone)- regulates growth of gonads & reproductive activities
Posterior Pituitary(Neurohypophysis) Antidiuretic hormone (ADH) Oxytocin What hormones are released by the posterior pituitary signaled by the hypothalamus? ____________ & ____________.
ANTERIOR PITUITARY HYPERFUNCTION DISORDERS • ETIOLOGY • Primary: defect in gland itself -releases a particular hormone that is too much or too little. • Secondary: defect is somewhere outside of gland i.e. GHRH from hypothalamus TRH from hypothalamus
PITUITARY TUMORS • 10% OF ALL BRAIN TUMORS • What diagnostic tests diagnose a pituitary tumor? • Tumors usually cause hyper release of hormones *Determined by symptoms presented; evaluate serum/urine hormone levels; stimulation/suppression tests for hormone levels; CT, MRI, etc
ANTERIOR PITUITARY HYPERFUNCTION • What happens if: • TOO MUCH secretion of prolactin (prolactinoma)? • TOO MUCH release of Lutenizing Hormone (LH)? • Too much growth hormone secretion? • Which goolish character on the Addam’s Family had too much GH secretion Anovulation; menstrual irregularities; galactorrhea “Polycystic ovary syndrome;, due to effect on corpus lutea GIGANTISM IN CHILDREN; ACROMEGALY IN ADULTS
Effects of growth hormone. A, Comparison of (from left to right) gigantism, normal, and dwarfism. B and C, The patient’s hands and face show; Clinical signs of acromegaly. D, Acromegaly. Excessive secretion of growth hormone in the adult caused characteristic malocclusion of the teeth resulting from the overgrowth of the mandible.
TOO MUCH GROWTH HORMONE • GIGANTISM IN CHILDREN • skeletal growth; may grow up to 8 ft. tall; > 300 lbs • ACROMEGALY IN ADULTS • enlarged feet/hands, thickening of bones, prognathism(jaw projects forward), diabetes, HTN, wt. gain, H/A, • Visual disturbances, diabetes mellitus
ACROMEGALY IN ADULTS • progessive change in facial features • Hand in acromegaly; normal hand
What assessment findings would the nurse document? What priority health risks associated with acromegaly?
Video-You Tube Lecture “Effects of GH Deficiency in Adults” You Tube-Pituitary Giantism/Agromegaly “Egor” the Giant Video You Tube-Pituitary Giantism- Robert Wadlow “Worlds Tallest Man” died age 22
Cont. Hyperfunction of the Anterior Pituitary- An individual has a tumor of anterior pituitary gland which causes excess ACTH secretion • What “disease” is this? • What signs and symptoms are likely to be found? Cushing’s disease- condition in which pituitary gland releases too much adrenocorticotropic hormone (ATCH). Cushing's disease- a form of Cushing syndrome See next slide for Video- Remember this one-see adrenal disorders
MEDICAL INTERVENTIONS PITUITARY TUMOR • *Medications (goal…...reduce GH levels) • Somatostatin analogs (octreotide) • GH receptor antagonists (Pegvisomant) • Dopamine agonists (cabergoline) Dostinex *inhibits prolactin (prolactinoma) • FYI- If inadequate GH prior to puberty- what “condition” will this individual have? what drug might be given to treat? Pituitary Dwafism (panhypopituitarism)- give GH (somatostatin)
MEDICAL INTERVENTIONS PITUITARY TUMOR/REPLACEMENT THERAPY Radiation therapy External radiation- bring down GH levels 80% of time Steriotactic radiosurgery- Click to view You Tube video Risk post-procedure-increased risk for seizures
Neurosurgery: • Transsphenoidal hypophysectomy • Most commonly used approach • Incision thru floor of nose into sella turcica.
Newer Method-EndoscopicTranssphenoidal Hypophysectomy New Method Click to view! • No incisions ! • Less recovery time • Fewer complications
Posterior Pituitary-(Neurohypophysis) ADH (vasopressin) and oxytocin Name the hormones released by posterior pituitary when signaled by hypothalamus!
ADH (Vasopressin) • secreted by cells in hypothalmus-stored in posterior pituitary • acts on distal & collecting tubules of kidneys making more permeable to H20 • volume excreted • ADH is released when? • ADH has vasoconstrictive or vasodilation properties? With decreases blood volume, increased concentration of Na+ or other substances (drugs as opiooids, thiazide diuretics) also, pain, stress vasocontrictive
Oxytocin • Controls lactation & stimulates uterine contractions • ‘Cuddle hormone’Research links oxytocin and socio-sexual behaviors
Posterior Pituitary Disorders • SIADH (TOO MUCH ADH!!) • Numerous causes: • *Small cell lung cancer , other types cancer • CNS disorders • *Medications as, thiazide diuretics, opioids, general anesthetics, tricyclic antidepressants, others • Miscellaneous
SIADH (Syndrome of Inappropriate Antidiuretic Hormone Secretion)
If too much ADH, what clinical signs and symptoms are “typical”? Weight gain urine output serum Na levels (less than120mEq/L) weakness muscle cramps H/A
SIADH-if hyponatremia worsens-high risk neuro manifestations • lethargy • decrease tendon reflexes • *seizures-life threatening! (if serum Na less than 120mEq/L)
Posterior Hypopituitary-ADH disorders Etiology: (50% idiopathic) • *Central- neurogenic- i.e. brain tumors • Nephrogenic - inability of tubules to respond to ADH • Psychogenic- Diabetes Insipidus-(DI) (too little ADH)
What Clinical Manifestations-DI? • Polydipsia • Polyuria (10L in 24 hours) • Severe fluid volume deficit • wt loss • tachycardia • constipation • shock
FOCUS-DISORDERS OF ADRENAL GLANDS • Adrenal Cortex • Adrenal Medulla How Stuff Works
ADRENAL CORTEX • Think • Salt • Sugar • Sex SUGAR
SALT • Mineralocorticoids (F & E balance) • Aldosterone (renin from kidneys controls adrenal cortex production of aldosterone) • Na retention • Water retention • K excretion
Question: If Na level is low, does aldosterone promote renal reabsorption of sodium and excretion (loss) of potassium? YES or NO?? YES
SUGAR (Cortisol)- • GLUCOCORTICOIDS (regulate metabolism; critical in stress response) • CORTISOL responsible for control & metabolism of • CHO (carbohydrates) • amt. glucose formed • amt. glucose released • FATS-control of fat metabolism • Stimulates fatty acid mobilization from adipose tissue • PROTEINS-control of protein metabolism • stimulates protein synthesis in liver • protein breakdown in tissues • INFLAMMATORY and allergic response • immune system-more prone to infection
SEX • ANDROGENS • hormones which male characteristics • release oftestosterone • Seen more in women than men
What is the RELEASE OF GLUCOCORTICOIDS CONTROLLED BY ______ ACTH(adrenocorticotropic hormone) Produced in anterior pituitary gland
ACTH • Circulating levels of cortisol • levels cause stimulation of ACTH • levels cause dec. release of ACTH What type of feedback mechanism is this?? Negative
AFFECTED BY: • Individual biorhythms • ACTH LEVELS -HIGHEST 2 HOURS BEFORE AND JUST AFTER AWAKENING. • usually 5AM - 7AM • Gradually decrease rest of day • Stress- cortisol production and secretion
ADRENAL MEDULLA • Fight or flight • What is released by the adrenal medulla? CATECHOLAMINE RELEASE • Epinephrine • Norepinephrine
HYPER AND HYPOFUNCTION ADRENAL CORTEX HORMONES: Too much: Too little CUSHING’S Syndrome(TOO MUCH CORTISOL!) • secretion of cortisol from adrenal cortex • 4X more frequent in females • Usually occurs at 35-50 years of age *Cushing’s disease if due to inc ACTH secreting tumor from pituitary
ETIOLOGY: Cushing’s Syndrome • Due to • Excess of corticosteroids, particularly glucocorticoids: most common cause: • Iatrogenic administration of exogenous corticosteroids Prolonged adm. of coricosteroids • 85% of endogenous cases due to ACTH-secreting pituitary tumor (Cushing’s disease) • Other causes include • Adrenal tumors (Cortisol secreting neoplasm within adrenal cortex) • Ectopic ACTH production in tumors outside hypothalamic–pituitary– adrenal axis • :usually lung and pancreas tumors
SIGNS & SYMPTOMS: Cushing’s (review video) • protein catabolism • muscle wasting • loss of collagen support • thin, fragile skin, bruises easily • poor wound healing • s in CHO metabolism • hyperglycemia • Can get diabetes- • insufficient insulin production • Polyuria • s in fat metabolism • truncal obesity • buffalo hump • “moon face” • weight but strength
Cushigns-SIGNS & SYMPTOMS • immune response More prone to infection • resistance to stress • Death usually from infection Before Cushings After Cushings
SIGNS & SYMPTOMS: Cushing’s Syndrome! • Androgen secretion • excessive hair growth • acne • change in voice • receding hairline • Mineralocorticoid activity • ________ and _______ retention • Marked hypokalemia • b.p. from ________ water NA hypervolemia