Download
1 / 1
10 likes | 222 Views
Overview of Fast Track Surgery. Development of a Fast-Track Surgery protocol in gynaecological oncology Alison Brand 1,3 , Verinder Sidhu 3 , Letitia Lancaster 1, David Elliot 2

E N D
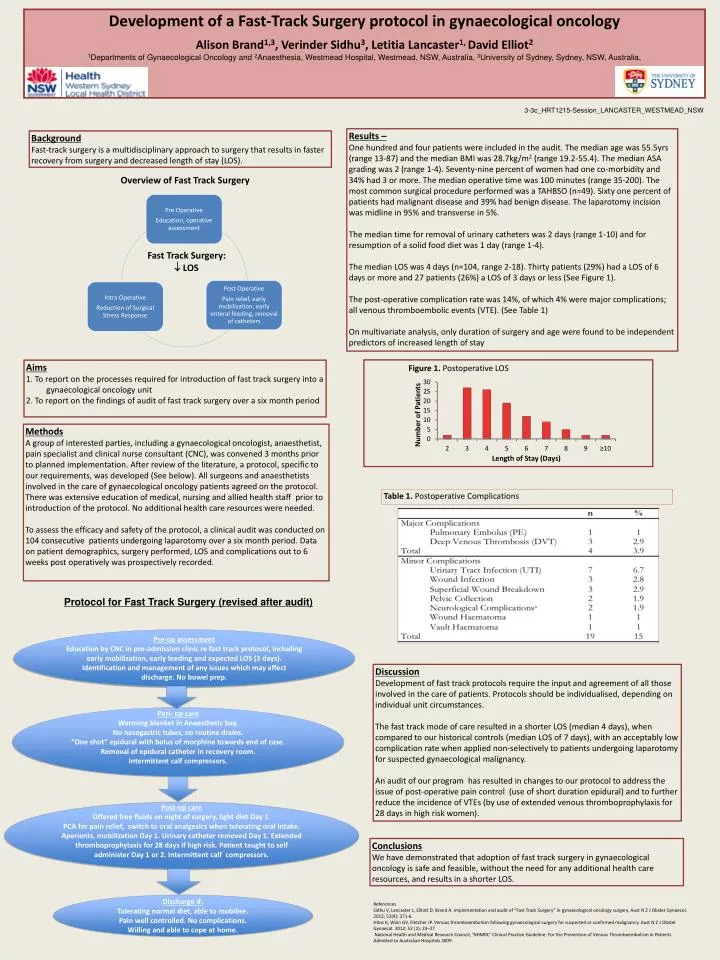
Overview of Fast Track Surgery Development of a Fast-Track Surgery protocol in gynaecological oncology Alison Brand1,3, Verinder Sidhu3, Letitia Lancaster1, David Elliot2 1Departments of Gynaecological Oncology and 2Anaesthesia, Westmead Hospital, Westmead, NSW, Australia, 3University of Sydney, Sydney, NSW, Australia, Fast Track Surgery: LOS 3-3c_HRT1215-Session_LANCASTER_WESTMEAD_NSW Results – One hundred and four patients were included in the audit. The median age was 55.5yrs (range 13-87) and the median BMI was 28.7kg/m2 (range 19.2-55.4). The median ASA grading was 2 (range 1-4). Seventy-nine percent of women had one co-morbidity and 34% had 3 or more. The median operative time was 100 minutes (range 35-200). The most common surgical procedure performed was a TAHBSO (n=49). Sixty one percent of patients had malignant disease and 39% had benign disease. The laparotomy incision was midline in 95% and transverse in 5%. The median time for removal of urinary catheters was 2 days (range 1-10) and for resumption of a solid food diet was 1 day (range 1-4). The median LOS was 4 days (n=104, range 2-18). Thirty patients (29%) had a LOS of 6 days or more and 27 patients (26%) a LOS of 3 days or less (See Figure 1). The post-operative complication rate was 14%, of which 4% were major complications; all venous thromboembolic events (VTE). (See Table 1) On multivariate analysis, only duration of surgery and age were found to be independent predictors of increased length of stay Background Fast-track surgery is a multidisciplinary approach to surgery that results in faster recovery from surgery and decreased length of stay (LOS). Figure 1. Postoperative LOS • Aims • 1. To report on the processes required for introduction of fast track surgery into a gynaecological oncology unit • 2. To report on the findings of audit of fast track surgery over a six month period Methods A group of interested parties, including a gynaecological oncologist, anaesthetist, pain specialist and clinical nurse consultant (CNC), was convened 3 months prior to planned implementation. After review of the literature, a protocol, specific to our requirements, was developed (See below). All surgeons and anaesthetists involved in the care of gynaecological oncology patients agreed on the protocol. There was extensive education of medical, nursing and allied health staff prior to introduction of the protocol. No additional health care resources were needed. To assess the efficacy and safety of the protocol, a clinical audit was conducted on 104 consecutive patients undergoing laparotomy over a six month period. Data on patient demographics, surgery performed, LOS and complications out to 6 weeks post operatively was prospectively recorded. Table 1. Postoperative Complications Protocol for Fast Track Surgery (revised after audit) Pre-op assessment Education by CNC in pre-admission clinic re fast track protocol, including early mobilization, early feeding and expected LOS (3 days). Identification and management of any issues which may affect discharge. No bowel prep. Discussion Development of fast track protocols require the input and agreement of all those involved in the care of patients. Protocols should be individualised, depending on individual unit circumstances. The fast track mode of care resulted in a shorter LOS (median 4 days), when compared to our historical controls (median LOS of 7 days), with an acceptably low complication rate when applied non-selectively to patients undergoing laparotomy for suspected gynaecological malignancy. An audit of our program has resulted in changes to our protocol to address the issue of post-operative pain control (use of short duration epidural) and to further reduce the incidence of VTEs (by use of extended venous thromboprophylaxis for 28 days in high risk women). Peri- op care Warming blanket in Anaesthetic bay. No nasogastric tubes, no routine drains. “One shot” epidural with bolus of morphine towards end of case. Removal of epidural catheter in recovery room. Intermittent calf compressors. Post-op care Offered free fluids on night of surgery, light diet Day 1. PCA for pain relief, switch to oral analgesics when tolerating oral intake. Aperients, mobilization Day 1. Urinary catheter removed Day 1. Extended thromboprophylaxis for 28 days if high risk.Patient taught to self administer Day 1 or 2. Intermittent calf compressors. Conclusions We have demonstrated that adoption of fast track surgery in gynaecological oncology is safe and feasible, without the need for any additional health care resources, and results in a shorter LOS. Discharge if: Tolerating normal diet, able to mobilise. Pain well controlled. No complications. Willing and able to cope at home. References Sidhu V, Lancaster L, Elliott D, Brand A. Implementation and audit of “Fast Track Surgery” in gynaecological oncology surgery. Aust N Z J ObstetGynaecol. 2012; 52(4): 371-6. Hitos K, Wain GV, Fletcher JP. Venous thromboembolism following gynaecological surgery for suspected or confirmed malignancy. Aust N Z J ObstetGynaecol. 2012; 52 (1): 23–27 National Health and Medical Research Council, ‘NHMRC’ Clinical Practice Guideline: For the Prevention of Venous Thromboembolism in Patients Admitted to Australian Hospitals 2009.






















