Download

1 / 14
140 likes | 169 Views
Explore the rationale, mechanism, and outcomes of BCG and IFN- combination therapy for bladder cancer, accentuating TH1 cytokine response, biocompatibility, and reduced toxicity with efficacy. Learn from published clinical trials and ongoing studies.

E N D
BCG Plus IFN-Combination TherapyRationale • Evidence of synergistic activity • Accentuates the TH1 cytokine response • Recombinant interferon alfa and BCG have complementary biologic activities • Infiltration of lymphocytes and NK cells to bladder (BCG) • Increased HLA expression on TCC cells (IFN-) • Increased cytolytic activity of cytotoxic T cells (IFN-) • Recombinant interferon alfa and BCG are biocompatible • Reduced dose of BCG may reduce toxicity while maintaining efficacy
BCG Plus IFN aMechanism of Action IFN-a (+) TH0 IL-12 Bladder Tumor Cell ExpressingActivation Markers and BCG Antigens (+) IFN-g (+) Activated Macrophage BCG TNF-a IL-2 TH1 IL 12 CTL
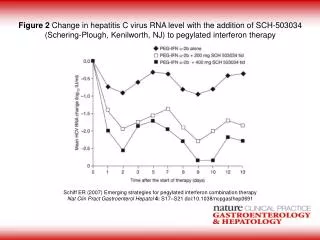
BCG Plus IFN -2bPublished Clinical Trials Tumor Median Study No. Type Regimen Dose Outcome F/U (Mo) Stricker, 1996 7 CIS IFN -2b + 10–100 MIU 86% CR 12 1/2-dose BCG* 60 mg 5 pTCC IFN -2b + 10–100 MIU 60% NED, 12 1/2-dose BCG 60 mg 40% PR Bercovich, 1995 18 pTCC Full-dose BCG* 120 mg RR = 28% 24 18 IFN -2b + 10 MIU RR = 22% 17 1/2-dose BCG 60 mg O’Donnell, 2001 40 Mixed, IFN -2b + 50 MIU 63% NED @ 12 mo 30 high risk 1/3-dose BCG† + 27 mg 53% NED @ 24 mo maintenance *Pasteur strain; †Connaught strain CR = complete response; NED = no evidence of disease; PR = partial response; RR = recurrence rate. Stricker P, et al. Urology. 1996;48:957. Bercovich E, et al. Arch Ital Urol Androl. 1995;67:257. O’Donnell MA, et al. J Urol. 2001;166:1300.
BCG Plus IFN -2b in BCG Failures • BCG failures (N = 40) • Median follow-up: 30 months; range, 15–52 months • High-risk population • 98% multifocal disease • 85% failed BCG within 6 months • 78% aggressive histology (CIS or grade 3, T1) • 63% multirecurrent disease (>2) • 52% failed >1 course of BCG; 48% failed 1 • 33% had long duration of bladder cancer (>4 years) • Cystectomy had already been offered to 22 O’Donnell MA, et al. J Urol. 2001;166:1300.
BCG Plus IFN -2b in BCG FailuresDisease-Free Survival 1.0 0.8 Median Follow-up = 30 Months 0.6 63% Fraction Free of Cancer 53% (Actual Disease Free = 55%) 0.4 0.2 No. Patients Available at Follow-up 40 40 40 39 37 31 25 15 10 8 4 2 0.0 48 0 4 8 12 16 20 24 28 32 36 40 44 Months After Treatment Initiation Reprinted by permission of Lippincott Williams and Wilkins from O’Donnell MA, Krohn J, DeWolf WC. Salvage intravesical therapy with superficial bladder cancer in whom bacillus Calmette-Guerin alone previously failed. J Urol. 2001;166:1300-1305.
BCG Plus IFN -2b in BCG FailuresRecurrences • 45% (18/40) had recurrence following BCG + IFN a-2b • 78% (14/18) recurrences were detected at 1st cystoscopy • 5 cases of muscle invasion, referred for cystectomy and/or chemotherapy + radiation • No early failures had metastasis or died of bladder cancer • 4 late recurrences (8, 21, 22, 24 months) • 2 low-grade, low-stage treated with TUR • 2 with disease outside bladder • No recurrences after 24 months or in the 46% who completed all 3 planned maintenance cycles O’Donnell MA, et al. J Urol. 2001;166:1300.
BCG Plus IFN -2b in BCG FailuresOther Observations • 42% (5/12) of those who required 2 induction regimens were long-term responders • Number of previous recurrences and tumor aggressiveness did not predict response • Patients who failed BCG twice did about as well as those who had failed BCG only once • Trend toward lower response rates in patients with previous relapse at <6 months of BCG or disease duration >4 years • Of 22 patients for whom cystectomy had already been recommended, 12 (55%) were disease free with normally functioning bladder at end of study O’Donnell MA, et al. J Urol. 2001;166:1300.
BCG Plus IFN -2b in BCG FailuresEfficacy Comparison With Historical Series 55 60 50 40 Disease Free at 2 Years (%) 30 23 20 20 12 8 10 0 BCG1 IFN a-2b2 Mitomycin C3 Valrubicin4 BCG + IFN a-2b5 1. Catalona WJ, et al. J Urol. 1987;137:220. 2. Williams RD, et al. J Urol. 1996;155(suppl):494A [abstract 735]. 3. Malmstrom PU, et al. J Urol. 1999;161:1124. 4. Steinberg G, et al. J Urol. 2000;163:761. 5. O’Donnell MA, et al. J Urol. 2001;166:1300.
BCG Plus IFN -2b in BCG-Naive Patients • N = 22 BCG-naive patients • Full-dose BCG + 50 MIU IFN a-2b • Disease free at 2 years: 68% O’Donnell MA, unpublished data cited in O’Donnell MA, et al. J Urol. 2001;166:1300.
BCG Plus IFN 2b Ongoing Randomized Trials Tumor Recurrence MedianStudy No. Type Regimen Dose Rate F/U (Mo) Esuvaranathan, 80 pTCC IFN -2b 10 MIU/ 10% 19 2000 + 1/3 BCG* 27 mg CIS vs 1/3 BCG 27 mg 30% vs full-dose 81 mg 50% BCG Lamm 100 TCC IFN -2b 50 MIU Ongoing Ongoing CIS + full-dose BCG vs full-dose BCG *Connaught strain Esuvaranathan K, et al. J Urol. 2000;163(suppl):152 [abstract 675].
BCG Plus IFN 2b SafetyNational Multicenter Phase II Trial • BCG/IFN has acceptable level of serious toxicity in comparison with BCG • Additional serious AEs with BCG/IFN • 10 cardiac events (8 not drug related) • 6 reversible neurologic events • Less risk of BCG sepsis (0.1% vs 0.4%) • Patients with previous BCG failure not at increased risk for toxicity O’Donnell MA, et al. Abstract 760. AUA 9th Annual Meeting; May 25–30, 2002; Orlando, Fla.
BCG/IFN is considered investigational Appropriate candidates may include: BCG Plus IFN 2b Candidates
BCG + IFN a-2b Combination TherapyConclusions • BCG + IFN a-2b combination therapy has synergistic immunomodulatory and antitumor activity (enhances the TH1 response) • In open-label trials, BCG + IFN a-2b combination therapy was well tolerated and allowed BCG dose reductions without compromising efficacy • BCG + IFN a-2b combination therapy is effective in patients who have failed ≥1 previous course(s) of BCG • Combination therapy may be considered prior to radical cystectomy in high-risk patients • Randomized controlled trials are under way