Download
1 / 56
700 likes | 2.52k Views
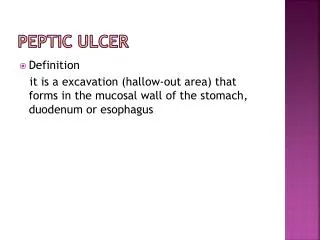
Recurrent Aphthous Ulcer. Etiology: Local altered immune response. Systemic etiologies include nutritional deficiencies (iron, B6, B12), diabetes mellitus, inflammatory bowel disease, immunosuppression. Biopsy will rule out other vesiculoulcerative disease. Recurrent Aphthous Ulcer.

E N D
Recurrent Aphthous Ulcer • Etiology: • Local altered immune response. • Systemic etiologies include nutritional deficiencies (iron, B6, B12), diabetes mellitus, inflammatory bowel disease, immunosuppression. • Biopsy will rule out other vesiculoulcerative disease.
Recurrent Aphthous Ulcer • Appearance: • Minor aphthous ulcer: <0.6 cm shallow ulceration with gray pseudomembrane and erythematous halo on non-keratinized mucosa. • Major aphthous ulcer: >0.5 cm ulcer, more painful, lasting several weeks to months; will scar.
Recurrent Aphthous Ulcer • Differential Diagnosis: • Herpes simplex virus. • Chemical/traumatic ulcer • Vesiculoulcerative diseases • Squamous cell carcinoma • Treatment: • Topical analgesics • Topical steroids
Inflammatory Conditions (Denture Related of the Oral Mucosa) • Inflammatory papillary hyperplasia • Epulis fissurata (inflammatory fibrous dysplasia) • Candidiasis
Inflammatory Papillary Hyperplasia • Etiology: • Poorly fitting denture • Occurs in more than 50% of Denture Wearers • Appearance: • Multiple small polypoid or papillary lesions. • Typically on hard palate, that produces a cobblestone appearance.
Inflammatory Papillary Hyperplasia • Etiology: • Poorly fitting denture • Occurs in more than 50% of Denture Wearers • Appearance: • Multiple small polypoid or papillary lesions. • Typically on hard palate, that produces a cobblestone appearance.
Inflammatory Papillary Hyperplasia (Papillomatosis) • Treatment: • Discontinue using denture • Surgical removal of hyperplastic tissue. • Occasionally tissue conditioner may reduce the problem, while reconstruction of new denture may be necessary.
Epulis Fissurata (Inflammatory Fibrous Dysplasia, Denture Granuloma) • Etiology: • Over-extended denture flanges. • Resorption of alveolar bone that makes the denture borders over-extended. • Appearance: • Hyperplastic granulation tissue surrounds the denture flange. • Pain, bleeding, and ulceration can develop.
Epulis Fissurata (Inflammatory Fibrous Dysplasia, Denture Granuloma) • Differential Diagnosis: • Verrucous carcinoma • Squamous cell carcinoma • Traumatic fibroma • Treatment: • Small lesions may resolve if flanges of denture are reduced. • Surgical excision is necessary prior to rebasing/relining of denture.
Candidiasis • Four fungal organisms: Candida albicans,Candida stellatoidea, Candida tropicalis, and Candida pseudotropicalis. • Candida albicans is most common. • Morphologically, presents in 3 forms: yeast cell, hypha and mycelium (last form is pathogenic phase). • Carriers of oral candida do not show the mycelial phase.
Etiology Mixed infection of Candida albicans, staphylococci and streptococci.
Classification of Oral Candidiasis • Acute pseudomembranous candidiasis (moniliasis, thrush). • Acute atrophic candidiasis (antibiotic sore tongue). • Chronic atrophic candidiasis (denture stomatitis). • Chronic hyperplastic candidiasis (candidal leukoplakia, median rhomboid glossitis). • Angular cheilitis • Chronic mucocutaneous candidiasis.
PAS Stained Candida Albicans Hyphae Embedded in The Oral Mucosa
Acute Pseudomembranous Candidiasis (Thrush) • Etiology: • Oral candidiasis • Appearance: • White slightly elevated plaques that can be wiped away leaving an erythmatous base. • Direct smear can be fixed and stained using PAS reagent to reveal the candida hyphea microscopically.
Acute Atrophic Candidiasis (Antibiotic Sore Tongue) • Etiology: • Oral candidiasis secondary to antibiotics or steroids. • Appearance: • Similar to thrush without overlying pseudomembrane: erythematous and painful mucosa. • Differential Diagnosis: • Erosive lichen planus. • Chemical erosion.
Chronic Atrophic Candidiasis (Denture Sore Mouth) • Etiology: • Most common form of oral candidiasis; candidal infection of denture as well. • Treatment should be directed towards mucosa and denture.
Chronic Atrophic Candidiasis (Denture Sore Mouth) • Appearance: • Mucosa beneath denture is erythematous with a well-demarcated border. • Swabs from the mucosal surface may provide a prolific growth, but biopsy shows few candida hyphae in spite of high serum and saliva antibodies to candida. • Differential Diagnosis: • Inflammatory papillary hyperplasia.
Chronic Hyperplastic Candidiasis(Candida Leukoplakia) • Etiology • Oral Candidiasis lesions should be considered as potentially premalignant. Treatment should be directed toward mucosa and Leukoplakia. • Appearance • Confluent leukoplakic plaques characterized by Candida invasion of oral epithelium with marked atypia.
Angular Cheilitis • Etiology: • Diminished occlusal vertical dimension • Vitamin B or iron deficiencies • Superimposed candidiasis • Affects approximately 6% of General Population • Appearance: • Wrinkled and sagging skin at the lip commisures. • Desiccation and mucosal cracking.
Angular Cheilitis • Differential Diagnosis: • Dry chapped lips. • Basal cell carcinoma. • Squamous cell carcinoma.
Angular Cheilitis • Rx: Nystatin-triamcinolone acetonide ointment. Disp: 15 gm tube. Sig: Apply to affected area after each meal and qhs. Concomitant intraoral antifungal treatment may be indicated.
Diagnostic Criteria • C.F.U. in Candidiasis can vary from 1,000/ml to 20,000/ml. • As an adjunct to saliva samples, smears stained with PAS. • Thus clinical manifestations, salivary culture and stained smears are needed to confirm a diagnosis of Candidiasis.
Candidiasis • Rx: Nystatin oral suspension 100,000 units/ml. Disp: 60 ml. Sig: Swish and swallow 5 ml qid for 5 min. • Rx: Nystatin ointment. Disp: 15 gm tube. Sig: Apply thin coat to affected areas after each meal and qhs. • Rx: Clotrimazole trouches 10 mg. Disp: 70 trouches Sig. Let 1 trouch dissolve in mouth 5 times daily.
Candidiasis • Rx for Dentures: Improve oral hygiene of appliance. • Keep denture out of mouth for extended periods and while sleeping. • Soak for 30 min in solutions containing benzoic acid, 0.12% chlorhexidine, or 1% sodium hypochlorite and thoroughly rinse.
Candidiasis • Apply a few drops of Nystatin oral suspension or a thin film of Nystatin ointment to inner surface of denture after each meal.
Rx for Refractory Candidiasis • Fluconazole 100 mg (20 tabs; 2 tabs stat, then 1 tab daily). • Itraconazole 100 mg (20 tabs; 1 tab bid). • 2-4 weeks of Ketoconazole 200 mg (20 tabs, 1 tab daily).
DIAGNOSIS AND MANAGEMENT OF XEROSTOMIA IN THE ELDERLY PATIENT:
XEROSTOMIA • Xerostomia (dry mouth) is defined as a subjective complaint of dry mouth that may result from a decrease in the production of saliva.
XEROSTOMIA • It affects17-29%of samples populations based on self-reports or measurements of salivary flow rates. • More prevalent inwomen. • Can cause significant morbidity and a reduction in a patient’s perception ofquality of life.
SALIVA • It keeps the teeth healthy by providing a lubricant, calcium and a buffer. • It also helps to maintain the health of the gums, oral tissues (mucosa) and throat. • It also plays a role in the controlof bacteria in the mouth.