Download
1 / 18
180 likes | 200 Views
Pre-operative MSU culture may help prevent, but stone culture helps predict, post-operative sepsis risk at PCNL. Cetti RJ, Boucher L, Ranasinghe W, McCahy P Monash Medical Centre, Melbourne, Australia. Introduction.

E N D
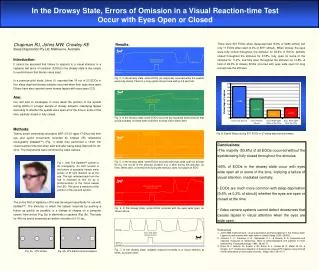
Pre-operative MSU culture may help prevent, but stone culture helps predict, post-operative sepsis risk at PCNL Cetti RJ, Boucher L, Ranasinghe W, McCahy P Monash Medical Centre, Melbourne, Australia
Introduction Percutaneous nephrolithotomy (PCNL) remains the preferred modality of treatment for large renal calculi >2cm [1]. [1] Turk C et al. EAU guidelines on Urolithiasis. Limited update 2014.
Introduction PCNL has an estimated complication rate of 20.5%, including a risk of sepsis approaching 5% even in the presence of a sterile pre-operative urine, and with the routine use of peri-operative antibiotics [2]. [2] Labate G et al. J Endourol 2011.
Introduction Intra-operative kidney stone culture may help in the post-operative septic patient to guide antibiotic treatment.
Introduction Intra-operative kidney stone culture may help in the post-operative septic patient to guide antibiotic treatment.
Introduction Intra-operative kidney stone culture may help in the post-operative septic patient to guide antibiotic treatment.
Aim The aim of this study was to evaluate the clinical benefit of pre-operative midstream urine culture (MSUC), stone analysis and stone culture (SC) in predicting sepsis risk at PCNL.
Methods A prospective analysis of pre-operative MSUC; SC, stone analysis and sepsis for all patients undergoing PCNL at Casey hospital, Monash Health, between May 2013 and May 2014.
Methods All patients were prospectively investigated with a MSUC. All patients with a positive result were prescribed appropriate antibiotics, and proceeded with PCNL when results were subsequently confirmed negative. Ceftriaxone 1g or Gentamicin 2.5mg/kg, and Ampicillin 1g iv. Antiseptic preparation was 10% povidone-iodine for the genitalia and 1% iodine/70%alcohol for the PCNL site.
Methods PCNL was performed with a single track, undertaken in the Casey modified supine position [3] under one surgeon (PM). McCahy P et al. J Endourol. 2013
Results 4 (7.5%) procedures were complicated with sepsis. 3/4 required intensive care treatment. 6 (11.2%) patients had a positive pre-operative MSUC. All were treated with appropriate pre-operative antibiotics. 5 (83.3%) of these patients still grew concordant pure growth micro-organisms from their stone culture, but none suffered post-operative sepsis. 13 (24.5%) patients had positive stone cultures, 8 of which had negative preoperative MSUC’s, including the 4/13 (30.8%) who developed post-operative sepsis.
Results- Predicting stone colonisation from preoperative MSUC.
Results-Predicting sepsis risk from stone culture. Sensitivity of SC to predict sepsis: 100% Specificity of SC to predict sepsis: 81.6% PPV: 30.8% NPV: 100%
Results • Statistically significant increased risk of stone colonisation in struvite compared to calcium oxalate stones (p=0.03) • Increased risk of sepsis in mixed uric acid stones compared with pure calcium oxalate stones (p=0.05)
Conclusions Pre-operative MSUC is mandatory. Pre-operative MSUC is, however, not sensitive for predicting positive stone culture and subsequent sepsis risk. Stone culture should be mandatory, to help direct post-operative antibiosis. Particularly in those patients with urate and struvite calculi.
Limitations Sample size. Tertiary referral. Data on DM, obesity, transfusion, dual access, operative time.