Download
1 / 16
160 likes | 292 Views
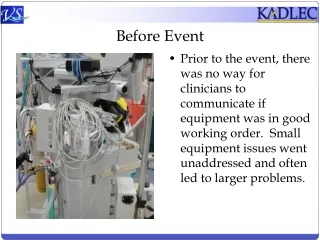
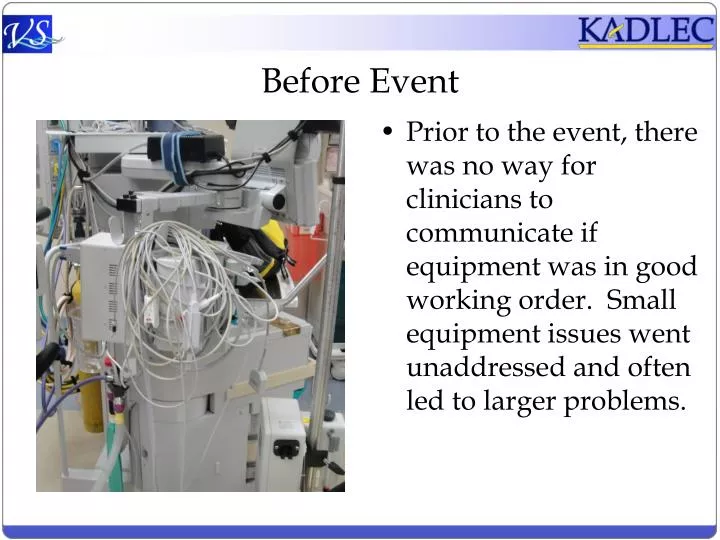
Before Event. Prior to the event, there was no way for clinicians to communicate if equipment was in good working order. Small equipment issues went unaddressed and often led to larger problems. After Event.

E N D
Before Event • Prior to the event, there was no way for clinicians to communicate if equipment was in good working order. Small equipment issues went unaddressed and often led to larger problems.
After Event • Green side provides sequence of Autonomous Maintenance steps to keep machine functioning properly. Green side exposed means the machine is fit for use.
After Event • The red side of the card allows clinicians to signal that equipment is not in proper working order. The most common failures are listed to eliminate diagnosis time needed by clinical engineering.
After Event • Red side exposed means equipment is unfit for use. All common errors are listed on the red side. Users denote reason for equipment failure and circle where failure is occurring on the diagram
After Event • As one of the deliverables, the team created a TPM manual for each machine which included guides for Operations, Schedule Maintenance, Trouble Shooting , and Critical Spares Replacement.
After Event • Prior to TPM implementation, scheduled maintenance logs were heavily text based and difficult to understand. The team designed a visual scheduled maintenance log based off of one found in an car maintenance manual. Now all team members know when equipment will be out of service.
AIDA AIDA After Event • Common equipment failures can now be corrected by the clinicians. The TPM manual contains simple step by step instructions on how to accomplish this.
Before Event • Prior to the event the staff were unfamiliar with the proper procedure for replacing critical spares on the machinery. As a result the Clinical Engineering staff were called for simple swapping of machine parts or changing batteries.
AIDA After Event • The team created documentation and processes around the replacement of critical spares. This among other documented processes were included in the TPM manual.
Before Event • Cords often cross crossed the OR floor creating opportunity for equipment failure.
Before Event • Improper cord and foot pedal management caused many false equipment alarms.
AIDA After Event • Convenient hooks were put in place for better cord and pedal management. Now clinicians can properly manage cords and pedals which used to be the source of many more serious equipment issues.
Before Event • On off switch at knee level caused loss of power during procedures. All captured images would be lost • Poor placement of PC contributed to accidental kicking of power cords causing issues during surgery
AIDA After Event • Guard placed on PC on/off switch to prevent accidental turn off during procedure • PC’s relocated to prevent accidental removal of cords
Before Event • Prior to the event there was no designated location to place broken equipment that required service. As a result broken equipment would remain in service.
AIDA After Event • The team selected and cleared an area and visually identified drop off locations where broken equipment is stored and removed from circulation. Clinical Engineering monitors these locations at least daily.


![[Event]](https://cdn2.slideserve.com/3738001/event-dt.jpg)