Download
1 / 34
340 likes | 358 Views
Explore the case of a 23-year-old female with Familial Hypercholesterolemia. Learn about advanced testing and treatment recommendations for this primary prevention scenario. Follow her journey through lipid profile assessments and personalized management strategies.

E N D
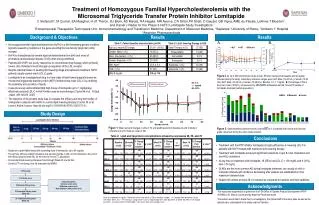
23 Year Old Female of Child Bearing Age with Familial Hypercholesterolemia Case category: Primary Prevention, Familial Hypercholesterolemia, Child Bearing Age History of present illness: 23 year old female of child bearing age with Familial Hypercholesterolemia. She is interested in advanced testing and treatment recommendations.
Lipid Profile Fasting: F NT = Not Tested
Other Labs Worth Noting Fasting: F NT = Not Tested
Labs (1 of 7) Traditional lipid profile suggests Familial Hypercholesterolemia. Most patients with this diagnosis will have high LDL-C and total cholesterol with normal HDL-C and triglycerides.
Labs (4 of 7) Patient is not on any therapies and this suggests hyperabsorption of sterols. At minimum she should AVOID any products containing PHYTOSTEROLS as she absorbs them and if absorbed may be more toxic than her own cholesterol. This also suggests, in addition to a statin for familial hypercholesterolemia, she will be a good candidate for Zetia if not able to get to goal on monotherapy. Would avoid high dose statin which can worsen hyperabsorption.
NMR LipoProfile • Insert NMR Lipoprofile 122111 SM88 Insert
NMR Interpretation • NMR confirms suspicion for Familial Hypercholesterolemia (FH). These patients have high LDL–P but no evidence of insulin resistance. Their LDL particles will be characteristically large. This is a very predictable pattern on NMR of a young patient with FH.
Questions to Consider Question 1: She is currently taking oral contraceptives. Does she have plans of childbearing in the next year? (She is open to pregnancy in the next year but does continue to take OCP.) Question 2: Do most family members on fathers side have hyperlipidemia? If Familial Hypercholesterolemia(FH) is present then autosomal dominant inheritance. This helps with diagnosing FH. Question 3: Open to taking medications for dyslipoproteinemia?
Initial Treatment & Management • As she is of child bearing age, start Niaspan 1500 mg/day to lower LDL-P as alternative to statin. • CRP was high and omega 3 index was slightly low at 6 (optimal >8-10%). Niaspan therapy may improve CRP. Recommend increasing consumption of omega 3 rich fish. • Start vitamin D3 5000 IU/day for vitamin D deficiency.
Discussion (1 of 5) Risk Factors: Hyperlipidemia Assessment: Familial Hypercholesterolemia
Discussion (2 of 5) Assessment: Familial Hypercholesterolemia (Continued)
Discussion (3 of 5) Assessment: Elevated CRP
Discussion (4 of 5) Assessment: APO E3E4
Discussion (5 of 5) Assessment: Vitamin D Deficiency
Follow Up on Niaspan 1500 (1 of 2) • Familial Hypercholesterolemia – Improved. • Currently taking Niaspan 1500 mg/day. • LDL-P lowered from 2111 to 1258. Apo B decreased from 152 to 86. Total cholesterol reduced to 230 from 291. LDL-C dropped from 191 to 111. Non-HDL-C lowered to 135 from 214. Triglycerides are normal at 50. HDL is normal at 77. • Insulin level and free fatty acids are higher at this visit, but may be due to Niaspan. There is no evidence of insulin resistance on NMR. • Sterol testing is abnormal. Will monitor and recheck levels. No need to change treatment, but avoid phytosterol supplements. Will add Zetia if LDL-P increases. No need to add now as LDL-P is close to goal. • Continue therapy.
Follow Up on Niaspan 1500 (2 of 2) • Elevated CRP – Improved. • CRP lowered from 3.0 to 1.9. • LpPLA2 and MPO remain normal. • Omega 3 index is low at 5.4%. Optimal is >8-10%. • Highest sources of Omega 3 come from Atlantic salmon, herring, mackerel, or Bluefin tuna. • Start Lovaza 1-2 g/day. She could also use an omega 3 product over the counter that provides 2 grams of EPA/DHA. • Vitamin D Deficiency – Improved. • Currently taking vitamin D3 5000 IU/day. • Levels increased from 20 to 53. • Patient notes less fatigue. • Continue supplements.
NMR LipoProfile • Insert NMR Lipoprofile 030812 SM88 Insert
Clinical PearlsNiaspan as Monotherapy Niaspan is very effective as an LDL-P lowering agent. It can be used as monotherapy in women of child bearing age as an agent to lower LDL. Due to fact that Niaspan does not lower LDL cholesterol as much as LDL particle concentration, it is not often used as a LDL Lowering agent of choice. However, the effect on LDL–P is excellent and very appropriate to use in this special population.
Treatments that Alter Cholesterol Content of LDL Change LDL-C and LDL-P Differentially • LDL Particles (LDL-P) decreases more with: • niacin • fibrates • metformin • pioglitazone • omega 3 FAs • exercise • low carb diet • LDL Cholesterol (LDL-C) decreases more with: • statins • statin + ezetimibe • Bile acid sequestrates • estrogen replacement therapy • low fat, high carb diet
Clinical PearlsPhytosterol Supplements It is important to not take phytosterols without knowing sterol absorption status. Phytosterols are commonly taken by patients, such as Cholestoff, because they state they lower LDL Cholesterol. These supplements may be hidden in orange juice that “lowers your cholesterol”, margarines etc. Even AHA guidelines recommend their use. In this patient, it would be dangerous to supplement with these products as she is a hyperabsorber of sterols. It would not be uncommon at all in a women of child bearing age to take these or have her health care professional recommend them. This message needs to be understood and more sterol testing needs to be done or avoid use of these products all together. There is no evidence in outcome studies that phytosterol supplementation has any effect.