Download
1 / 44
450 likes | 747 Views
Clinical Evaluation of Glomerular Filtration. S.P. DiBartola, DVM D.J. Chew, DVM. The ideal substance to measure GFR would …. Be freely filtered at the glomeruli Not be bound to plasma proteins Not be metabolized Be non-toxic Be excreted only by the kidneys

E N D
Clinical Evaluation of Glomerular Filtration S.P. DiBartola, DVM D.J. Chew, DVM
The ideal substance to measure GFR would … • Be freely filtered at the glomeruli • Not be bound to plasma proteins • Not be metabolized • Be non-toxic • Be excreted only by the kidneys • Be neither reabsorbed nor secreted by the renal tubules • Be stable in blood and urine • Be easily measured
Clinical Assessment of GFR • BUN • Serum creatinine • Creatinine clearance (endogenous or exogenous) • Sodium sulfanilate • Radioisotopes
Essential terminology • Renal disease • Renal failure • Azotemia • Uremia
Renal disease • Implies the presence of histologic lesions in the kidney but does not specify any degree of renal dysfunction
Renal failure • Implies that 75% of the total nephron population has become non-functional but does not necessarily imply underlying histologic lesions
Azotemia • Increased concentration of non-protein nitrogenous waste products (e.g. urea, creatinine) in the blood
Azotemia • Pre-renal: due to reduced renal perfusion • Renal: due to renal parenchymal disease • Post-renal: due to impaired elimination of urine from the body
Uremia • The constellation of clinical and biochemical abnormalities associated with a critical loss of functioning nephrons • Includes the extra-renal manifesations of renal failure
Blood urea nitrogen (BUN) • Dogs: 8-25 mg/dL • Cats: 15-35 mg/dL • Horses: 10-27 mg/dL • Cattle: 5-23 mg/dL Normal values may vary among laboratories
Production of urea • Synthesized in liver using NH3 derived from amino acids of endogenous (body) or exogenous (dietary) proteins • Not produced at a constant rate (affected by protein intake) NH4+ + CO2 + 3ATP + 2H2O + aspartate urea + 2ADP + 2Pi + AMP + PPi + fumarate + 2H+
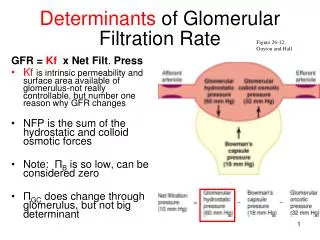
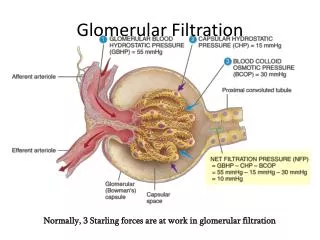
Distribution and excretion of urea • Freely permeable and distributed throughout total body water • Renal excretion most important • Filtered by glomeruli • Passively reabsorbed in renal tubules depending on tubular flow rate • Not secreted by renal tubules • Not excreted at a constant rate (high protein meal transiently increases GFR)
Measurement of urea • Technically easy and reproducible • Measured by diacetylmonoxamine or urease methodology • Urease methodology most specific and accurate (used on Hitachi autoanalyzer) • Dipstrip (e.g. Azostix) methods not very accurate
Abnormal BUN concentration • Non-renal factors • Renal factors • Pre-renal (e.g. dehydration, heart failure, shock) • Renal (e.g. parenchymal renal disease) • Post-renal (e.g. urethral obstruction, ruptured bladder)
Abnormal BUN: Non-renal factors • Increased BUN • High protein meal • Hemorrhage into gastrointestinal tract • Increased catabolism • Drugs (glucocorticoids, azathioprine, tetracycline) • Decreased BUN • Low protein diet • Severe liver disease or portosystemic shunt • Drugs (anabolic steroids)
Creatinine • Dogs: 0.3-1.2 mg/dL • Cats: 0.8-1.8 mg/dL • Horses: 1.0-1.8 mg/dL • Cattle: 0.6-1.5 mg/dL Normal values may vary among laboratories
Production of creatinine • Non-enzymatic breakdown product of phosphocreatine in muscle • Produced at a relatively constant rate based on age, gender, and muscle mass • Not affected by diet
Distribution and excretion of creatinine • Freely permeable and distributed throughout total body water • Renal excretion most important • Filtered by glomeruli • Not reabsorbed by renal tubules • Not secreted by renal tubules • Excreted at a relatively constant rate
Measurement of creatinine • Usually measured by alkaline picrate method (used on Hitachi autoanalyzer) • Measures creatinine and non-creatinine chromagens
Measurement of creatinine: Non-creatinine chromagens • May constitute up to 50% of measured “creatinine” at normal serum creatinine concentrations (but progressively less as renal function declines) • Do not appear in urine (affects clearance calculations) • Special techniques to circumvent them are not in common use by clinical laboratories
Abnormal serum creatinine concentration • Non-renal factors (usually transient) • Renal factors • Pre-renal (e.g. dehydration, heart failure, shock) • Renal (e.g. parenchymal renal disease) • Post-renal (e.g. urethral obstruction, ruptured bladder)
Abnormal serum creatinine concentration: Non-renal factors • Increased creatinine (usually transient) • Massive muscle necrosis • Prolonged strenuous exercise • Decreased creatinine • Severe loss of muscle mass • Small body size • Young age
Relationship between BUN or creatinine and % functional nephrons is a “rectangular hyperbola” • Large changes in GFR “early” in renal disease cause small changes in BUN or creatinine • Small changes in GFR late in renal disesae cause big changes in BUN or serum creatinine
Implication of azotemia • In a “steady state” and when non-renal factors have been eliminated from consideration, an increase of BUN or creatinine above normal implies that at least 75% of the nephrons are not functioning
Magnitude of azotemia does NOT … • Differentiate pre-renal, renal, and post-renal processes • Differentiate acute from chronic processes • Differentiate reversible from irreversible processes • Differentiate progressive from non-progressive processes
BUN vs serum creatinine • Both are relatively insensitive indicators of renal function (one is not more sensitive than the other) • Serum creatinine is affected by fewer non-renal variables • Creatinine is not affected by passive renal tubular reabsorption
BUN/creatinine ratio • May be increased in pre-renal azotemia (e.g. dehydration) due to increased tubular reabsorption of urea at slower tubular flow rates • May be increased in post-renal azotemia caused by ruptured bladder due to easier reabsorption of urea across peritoneal membranes
Localization of azotemia • Must consider: • History • Physical examination findings • Urine specific gravity before fluids or drugs that may interfere with concentrating ability • Patient’s response to fluid therapy
Localization of azotemiaExample 1 • Hx: Persistent vomiting • PE: 10% dehydrated • Lab: BUN 70 mg/dL; USG 1.054 • Response to fluids: BUN 20 mg/dL • Conclusion: Pre-renal azotemia
Localization of azotemiaExample 2 • Hx: Weight loss, lethargy, anorexia, vomiting • PE: 10% dehydrated • Lab: BUN 175 mg/dL; USG 1.013 • Response to fluids: BUN 75 mg/dL • Conclusion: Pre-renal and renal azotemia
Localization of azotemiaExample 3 • Hx: Lethargy, vomiting • PE: 10% dehydrated • Lab: BUN 70 mg/dL; USG 1.013 • Response to fluids: BUN 20 mg/dL • Conclusion: Pre-renal azotemia, underlying renal disease
Concept of clearance • Volume of plasma that would have to be filtered by the glomeruli in one minute to account for the amount of that substance appearing in the urine each minute under steady state conditions • Volume of plasma that contains the amount of the substance excreted in the urine in one minute under steady state conditions
Clearance = UxV/Px • Where, • Ux = urine concentration of x (mg/dL) • Px = plasma concentration of x (mg/dL) • V = urine output (mL/min)
Relationship of clearance to GFR • In a steady state, for a substance handled only be the kidneys that is neither reabsorbed nor secreted: • Amount filtered = amount excreted • GFR Px = Ux V • GFR = UxV/Px • Thus, the clearance of a substance that is neither reabsorbed nor secreted is equal to GFR
Relationship of clearance to GFR • If X is neither reabsorbed nor secreted, clearance = GFR • If X is reabsorbed, clearance < GFR • If X is secreted, clearance > GFR
Inulin clearance • Inulin is a polymer of fructose that meets all of the criteria for the ideal substance to measure GFR • Inulin clearance is the “gold standard” for GFR determination • Inulin must be continuously infused into the animal to achieve a steady state concentration in plasma
Creatinine clearance • Creatinine is produced endogenously at a constant rate • It is not metabolized • It is excreted by the kidneys by glomerular filtration • It is neither reabsorbed nor secreted by the renal tubules • Creatinine clearance can be used to estimate GFR
Endogenous creatinine clearance • Requirements: • Accurately timed collection of urine • Body weight • Serum and urine creatinine concentrations • Normal = 2 to 5 ml/min/kg • Underestimates GFR (compared to inulin clearance) due to non-creatinine chromagens in blood (Px increased)
Exogenous creatinine clearance • Serum creatinine increased 10-fold by administration of creatinine • Minimizes effect of non-creatinine chromagens • More closely approximates inulin clearance • Technically more difficult than endogenous creatinine clearance
Indications for creatinine clearance • Suspicion of renal disease in a non-aoztemic patient with PU/PD
Sodium sulfanilate • Excreted solely by glomerular filtration • Plasma half-life is an indicator of GFR • Administered IV and heparinized blood samples collected at 30, 60 and 90 min • Normal values: 30-80 min (depending on species)
Sodium sulfanilate • Advantage: Urine samples not required • Disadvantage: No numerical value for GFR is obtained Seldom used in clinical evaluation of renal function in domestic animals
Radioisotopes • Used to determine glomerular filtration, renal plasma flow, and filtration fraction in domestic animals • Advantages • Do not require collection of urine • Not time consuming • Disadvantages • Use of radioactivity • Require special equipment and expertise
Radioisotopes • Glomerular filtration rate • 125I-iothalamate • 51Cr-ethylenediaminetetraacetic acid (EDTA) • 99mTc-diethylenetriaminepentaacetic acid (DTPA) • Renal plasma flow • 131I-iodohippurate • 3H-tetraethylammonium bromide