Download
1 / 20
310 likes | 1.19k Views
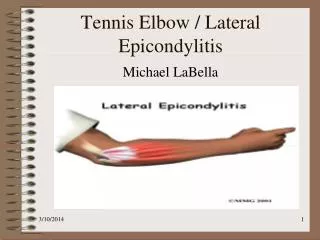
Tennis elbow. Lateral epicondylitis ; lateral tennis elbow; lateral stress syndrome.

E N D
Lateral epicondylitis; lateral tennis elbow; lateral stress syndrome Tennis elbow is a lesion affecting the tendinous origin of the wrist extensor. Most commonly involves the extensor carpi radialis brevis (ECRB), occasionally, the anterior edges of the extensor communis, the extensor radialis longus, and rarely the origin of the extensor carpi ulnaris. We can say that the lesion may be tenoperiosteal, tendinous or musculotendinous.
Etiology: A direct blow to one of the epicondylar areas, or a sudden extreme effort or activity. Some individuals have a heritable constitutional factor that predispose to profuse or generalized tendinitis. Any activity causing repeated, gradual stresses to the wrist extensors, primarily the ECRB, can lead to the acute or chronic overuse syndrome (tennis elbow).
Overuse: • The ECRB is stretched over the radial head when the elbow is extended and fully pronated. This fulcrum effect may partially explain its susceptibility to chronic inflammation at or near its attachment. • Overuse in some strenuous occupation producing strain to the muscles near the elbow by repetitive movements. This repetitive muscle contraction, chronically overloading the ECRB in its most vulnerable position, leads to fatigue and microtrauma.
Incidence: It is prevalent in those over 35 years of age, both male and female are equally affected Pathology: • With aging the tendons are less able to attenuate forces , and decreased levels of glycosaminoglycans (GAG) lead to decreased extensibility. • Soft tissue inflammation, tear or degeneration develops, The inflammatory response is an attempt to increase the rate of tissue production to compensate for the increased rate of tissue micro damage. • Healing is slow and the lesion tends to become chronic because the blood supply isrelatively poor in middle age. The tendon is invaded by fibroblasts and vasculargranulation like tissue (angiofibroplastic hyperplasia).
Course: Prolonged course, with exacerbation and remissions often lasting up to 2 years. • Evaluation: 1- Onset is usually gradual and is related to increased activity of the wrist extensor. Symptoms include a dull ache at rest, which may be converted to sharp pain during activity. 2- Palpation: Tenderness over the lateral epicondyle and occasionally tenderness in the muscle belly. Temperaturemay be slightly elevated over the epicondyle.
3-Active movement: . Generally painless. In severe involvement, pain may be felt during active wrist flexion with the elbow extended because of stretching of the ECRB. 4- Passive movement: Full wrist extension with ulnar deviation, forearm pronation and elbow extension, should reproduce pain. 5- Special tests: . Resisted wrist extension with the elbow extended reproduce pain. a) Painful resisted extension of the middle and ring fingers indicate affection of the extensor digitorum communis.
b) Painful resisted wrist extension and radial deviation points to ECRL and ECRB. c) Passive flexion of the wrist while elbow is extended and forearm is pronated thereby stretching the tendinous insertion. A positive test elicits pain at the common origin. 6-Accessory movements: Abduction in fully extended position, usually show some restriction of movement and reproduce pain.
Acute Lateral Epicondylitis: Treatmentof these patients involves progression to the chronic state by resolving the acute inflammation as follows: 1-Ice: two to three times a day over the site of inflammation. 2-Rest: Wrist immobilization (cock-up splint). Activities that aggravate the condition should be eliminated (grasping, pinching, tennis, and knitting). 3-Gentle active wrist flexion, forearm pronation with elbow extension, stretching, and general wrist and forearm range of motion exercise, two to three times a day. 4-Iontophoresis or phonophoresis may help resolve the inflammatory process
Chronic Lateral Epicondylitis: 1-Restriction of the heavy activities that stress the tendon. 2-Underwater ultrasound assists in the resolution of inflammatory exudates by increasing local blood flow. 3-Deep transverse friction massage is necessary to promote proper orientation of immature collagen along the lines of stress, parallel to the muscle fibers. 4-Iontophoresis or phonophoresis 5-Strength and mobility should be restored and the patient should gradually resume activities. Mobilization is indicated in case of: i) Loss of full passive elbow extension. ii) Loss of normal accessory movements with a painful limitation in the extension adduction rang .
6- The patient should be taught preventive measures, including proper protection in inclement weather, limiting activity to reach fatigue, and selection of proper equipment. 7- Counter-force brace: also called arm band or epicondylar splint, it is a non elastic fabric lined with foam rubber to prevent slipping. The counter-force concept limit muscular expansion, and reduces the contraction force of the muscle
The characteristics of this band: 1-It must be wide enough 3 to 3.5 inches. 2-It should be applied by tensing the muscles of the arm then placing the band tightly. If it is applied while the muscles are relaxed it may cut off the circulation 3-The band should be comfortable with the forearm relaxed. 4-The band should not be put too proximally, but about 2 finger breadth distal to elbow flexor crease over the major muscle belly. 5-A pneumatic splint may be more comfortable, with the air bag centered over extensor muscles mass.
Exercise program: Stage I : Prepare for exercise with heat, ice or ultrasound. Isometric progressed through elbow flexion, neutral, and extension as pain permits. Progress to the second stage when maximal isometric contraction is possible in extension with no pain. Stage II : Prepare for exercise with heat and stretching.Isotonic exercise (concentric and eccentric) through a full range of motion, start with small resistance.
Stage III : Isotonic exercise for full range. Add wrist flexion and extension stretches, and ice down over the common extensor tendon after each session. Progress to next stage if there is no pain. Stage IV : Ensure adequate warm up (local heat or general exercises). Commence to functional exercises. Stage V : Build up intensity and time slowly. Continue home strengthening and stretching program. Use ice after heavy workouts :
N.BThroughout the physical therapy program, strength and range of motion of both shoulder and trunk should be maintained. Attention should be given to shoulder rotation range of motion, and to the weakness of both shoulder external rotators and abductors. The overall goal is to restore flexibility, strength, endurance, and coordination of the whole upper extremity.
Operative Treatment: Postoperative Rehabilitation: 1-The elbow is maintained in an elbow immobilizer for 6 days postoperative. 2-Gentle active motion in a warm shower for 1 week followed by a gradual return, to strength training, with protection by a lateral counter-force brace (usually fox the first week of strength training), 3-Start easy strokes about 6 weeks from the time of surgery. 4-Full return to competition, even at a world class level, averages 4 to 5 months.
GOLFER'S ELBOW Medial Epicondylitis; Medial Tennis Elbow; Epitrochleitis .
Definition: Medial tennis elbow involves primarily the flexor origin at the medial epicondyle. Etiology: It is an overuse syndrome in the throwing sports, where it may be related to repetitive valgus stress along with pronation and wrist flexion. Golfing with excessive driving, or by mishittingthe ground. Racket sports due to the wrist action. Also in baseball pitching, and in pull-through phase of swimming strokes. Occupations that require a strong hand grip and an adduction movement of the elbow. It occurs in middle aged subjects involved in these activities.
Evaluation: 1-Tenderness on palpation felt under the medial epicondyle. 2-Pain on resisted pronation of the forearm. 3-Pain on stretching the flexor muscles group by fully extending the forearm from supine position, and then passively hyper extending the wrist. 4- Pain on resisted wrist flexion and ulnar deviation.
Treatment: This is similar to that outlined for lateral epicondylitis; namely rest, medication, mobilization, counter-force brace, ultrasonic, heat and ice, stretching and strengthening. Failure of conservative treatment will open door for surgery, mainly medial tenotomy. Postoperative program of physical therapy similar to that used for tennis elbow is used. Full return for competition takes at least 5 to 6 months for medial elbow tendinitis.