Download
1 / 37
410 likes | 1.09k Views
The Elbow and Forearm. The Elbow. A hinge joint performing flexion, extension, pronation, and supination Anatomy Humerus Lateral/Medial Epicondyle Olecranon Fossa. The Elbow. Anatomy Radius lateral bone of the forearm Radial Tuberosity Radial Styloid process Ulna

E N D
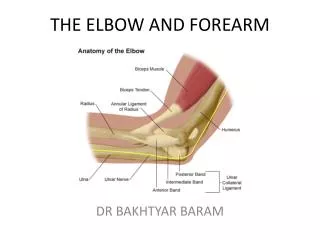
The Elbow • A hinge joint performing flexion, extension, pronation, and supination • Anatomy • Humerus • Lateral/Medial Epicondyle • Olecranon Fossa
The Elbow • Anatomy • Radius • lateral bone of the forearm • Radial Tuberosity • Radial Styloid process • Ulna • Medial border of the forearm • Semilunar notch • Olecranon process
The Elbow • Articulations • Flexion and Extension • Humeroulnar joint • Humeroradial joint • Supination and Pronation • Humeroradial joint • Superior and inferior Radioulnar joints
The Elbow • Ligamentous support • Ulnar collateral Lig. (UCL) • Divided into sections • Anterior Oblique band • Transverse Oblique band • Posterior oblique band
The Elbow • Ligamentous Support • Lateral Ulnar collateral Lig. (LUCL) • Radial Collateral Lig. (RCL) • Annular Ligament • Interosseus Membrane
The Elbow • Supporting Structures • Types • Static Structure • Dynamic Structure
Static Structures • Includes • Fibrous Capsule • Collateral Ligaments • Synovial membrane • Fat pads • At the Olecranon Fossa (largest) • Over the radial and coronoid fossae (2 small fat pads)
Dynamic Structures • Supinator muscle - supports lateral joint and serves as false ligament • Other muscle around elbow joint
Cubital Fossa • Passing within the fossa is the • Brachial artery • Median Nerve • Biceps Tendon • Musculocutaneous Nerve • This is called the Triangular Space
Carrying Angle • The way the forearm goes outward when at ones side. • Caused by the size of the trochlea. • Valgus (outward angulation) of 5-15 degrees is normal • being greater in females. • Cubitus Valgus/Varus • Gunstock deformity • A deformity of the elbow, resulting from condylar fracture at the elbow in which the forearm deviates toward the midline of the body when extended.
Isoceles Triangle • Medial and lateral epicondyles, Olecranon process. Forms a triangle in flexion and lines up in extension • Boarded laterally by the Brachioradialis and medially by the pronator teres
Eating Angle • Due to the carrying angle hand goes straight to the mouth when elbow is flexed.
Observation • Note the carrying angle • Note Cubitus valgus and/varus • excessive swelling • Look for normal bony and soft tissue contours • Functional position • 90 degrees of flexion with hand in neutral
Range of Motion • AROM • Flexion - 135-145 degrees • Extension - 0-10 degrees • Supination - 90 degrees • Pronation - 80-90 degrees
Circulation • Brachial Artery • The pulse of the brachial artery can be felt directly medial to the biceps tendon insertion
Peripheral Nerve Injuries • Median Nerve (C6-C8,T1) innervates wrist & finger flexors & pronates forearm • Pinched or compressed as it passes under the Lig. of Struther • Weakness of the pronator teres, and motor and sensory loss • Referred as Humerus Supracondylar Process Syndrome
Peripheral Nerve Injuries • Pronator Teres Syndrome • As the median nerve passes through the two heads of the pronator teres it can be compressed • In this case the pronator teres remains normal and the other muscles supplied by the median nerve become involved down the median nerve’s motor distribution. • The motion of pronation is possible but weak • Tested with Pronator Teres Syndrome Test: + sign is tingling or paresthesia in the median nerve distribution of the forearm and hand
Pronator Teres Syndrome Test • The patient stands with the elbow in 90 degrees of flexion. • The practitioner then places one hand on the client's elbow for stabilization and the other hand grasps the client's hand in a handshake position. • The client holds this position as the practitioner attempts to supinate the client's forearm (forcing the client to contract the pronator muscles). • While holding the resistance against pronation, the practitioner extends the client's elbow • If the client's pain or discomfort is reproduced, there is a good chance of median nerve compression by the pronator teres
Pronator Teres Syndrome • Pronator Teres Syndrome Test: In 90 degrees of elbow flexion the pronator teres muscle is weaker: a positive test is indicated by tingling or parenthesis in the median nerve distribution
Peripheral Nerve Injuries • Anterior Interosseus Nerve- Pinch Deformity • Sometimes pinched or entrapped as it passes the pronator teres, leading to impairment of • Flexor pollicis longus • Flexor digitorum profundus (lateral half) • Pronator Quadratus • Anterior Interosseous Nerve Syndrome or Kiloh-Nerin Syndrome- exhibited by pinch deformity: + sign is touching finger pulp-to-pulp instead of finger tip to finger tip • AIS causes no sensory loss because the AIN is a motor nerve
Peripheral Nerve Injuries • Ulnar Nerve (C7-C8, T1)- innervates flexors of wrist & finger, intrinsics of the fingers and thumb • Likely to be compressed or stretch in the Cubital tunnel • Compressed by • The Cubital Tunnel • Between the two heads of the flexor carpi ulnaris muscle
Peripheral Nerve Injuries • Radial Nerve (C5-C8, T1) innervates triceps, brachiolis, brachioradialis, supinator ,& extensor muscles of wrist and fingers • May be injured as it winds around behind the Humerus in the Radial Groove. • Damage can occur at time of injury or later when the nerve gets caught in the callus of fracture healing • The extensor muscle of the arm are supplied by the radial nerve and only the triceps get spared with this injury
Peripheral Nerve Injuries • Posterior Interosseous Nerve • Radial Tunnel Syndrome • The PIN can be compressed as it passes b/t the two head of the Supinator in the Arcade or Canal of Frohse. • Compression leads to functional involvement of forearm extensor muscles and drop wrist • No sensory deficit and may mimic tennis elbow
Elbow Pathology • Lateral Epicondylities/Radiohumeral Bursitis • Location: extensor carpi radialis brevis tendon or the extensor commounis tendon • Signs & Symptoms: • Pain & tenderness on the outer side of elbow • Pain or weakness with gripping activities • Pain with twisting motions of the wrist ( playing tennis, using a screwdriver, opening a door or jar) • Pain with lifting objects
Lateral Epicondylitis • Causes: • Chronic repetitive stress and strain to the muscles and tendons that attach the forearm muscles to the elbow • Sudden change in activity level or intensity • Incorrect grip • Incorrect grip size of racquet (often to large) • Incorrect hitting position or technique ( usually backhand; leading with the elbow • Using a racket that is too heavy
Radial Head Fractures • MOI: • FOOSH injury • Elbow Dislocation • Direct Blow to the area
Radial Head Fractures • Three Types or Classifications: • Type I: Nondisplaced • Type II Marginal radial fractures that are displaced • Type III: Comminuted Fractures involving the entire radial head
Elbow Dislocation • Very common in children and athletes • MOI: FOOSH injury • Direct blow or twisting injury to the elbow • Posterior Dislocations are most common(98%) • Seldom occur in isolation – are associated with fracture of the radial head (occur in 10%), Neurovascular involvement including brachial artery and median nerve
Elbow Dislocations • Signs and Symptoms: • Extreme pain, swelling, and inability to bend the elbow • Deformity with olecranon protruding posteriorly and inferiorly • Loss of elbow function • Severe pain when attempting to move the elbow • Numbness or paralysis in the forearm or hand below the dislocation from pinching , stretching, or pressure on the blood vessels or nerves • Decrease or absent pulse at the wrist
Olecranon Bursitis • Inflammation of the bursa located b/t the skin and tip of the ulna • Common in contact sports such as wrestling, football, volleyball
Olecranon Bursitis • Signs and Symptoms • Pain, tenderness, swelling, warmth, or redness over the olecranon process • Crepitaiton ( a crackling sound) on movement or touch • Fever when infected • Often painless swelling of the bursa
Valgus Stress TestUlnar Collateral Ligament • Patient: • Sitting with the humerus internally rotated and the elbow flexed to 10-25 • Examiner: • support the lateral elbow and with the fingers palpate the medial side of the joint • with the opposite hand grasp the distal forearm • Apply a valgus force to the joint (push elbow in pull wrist out) • Positive Test • increased laxity compared to the other side • Repeat test in 0 degrees of flexion
Varus Stress TestRadial Collateral Ligament • Same as Valgus test only push the elbow out and pull the wrist in
Moving Valgus Stress TestPartial Tear of the UCL • Patient: • sitting, shoulder abducted to 90, elbow flexed to the end of ROM • Examiner: • Apply a valgus force on the elbow and externally rotate the humerus • extend the elbow to 30 while maintaining a valgus force • move the elbow from extension into flexion while maintaining valgus force • Positive Test • pain at the medial elbow that occurs at the same point of ROM in extension and flexion
Cozen's TestTennis Elbow Test • The patient is seated, the practitioner stabilizes the elbow while palpating the lateral epicondyle. • The patient pronates and extends the wrist against resistance. • Pain with motion and or over the condyle is positive for tennis elbow.