Download
1 / 62
960 likes | 4.78k Views
Anatomy & Physiology of Eustachian Tube. Dr. Vishal Sharma. History & Embryology. Bartolomeus Eustachius first described it as pharyngo-tympanic tube in 1562. Antonio Valsalva named it Eustachian tube. Develops from tubo-tympanic recess , derived from endoderm of 1st pharyngeal pouch. .

E N D
Anatomy & Physiology of Eustachian Tube Dr. Vishal Sharma
History & Embryology • Bartolomeus Eustachius first described it as pharyngo-tympanic tube in 1562. • Antonio Valsalva named it Eustachian tube. • Develops from tubo-tympanic recess, derived from endoderm of 1st pharyngeal pouch.
Anatomy • 36 mm long in adults. • Directed anteriorly, inferiorly & medially from anterior wall of M.E., forming angle of 450 with horizontal & sagittal planes. • Enters naso-pharynx 1.25 cm behind posterior end of inferior turbinate.
Parts • Lateral 1/3 is bony • Medial 2/3 is fibro-cartilaginous. • Junction b/w 2 parts is isthmus, narrowest part of Eustachian Tube.
Anatomy of medial 2/3rd Cartilage plate lies postero-medially & consists of medial + lateral laminae separated by elastin hinge. Fibrous tissue + Ostmann’s fat pad lie antero-laterally.
Anatomy Muscle attachments: 1. tensor veli palatini or dilator tubae 2. levator veli palatini 3. salpingopharyngeus 4. tensor tympani Nerve supply: 1. Sphenopalatine ganglion 2. Mandibular nv 3. Tympanic plexus
Anatomy • Lining epithelium:respiratory epithelium • Arterial supply: ascending pharyngeal & middle meningeal arteries • Venous drainage:pharyngeal & pterygoid venous plexus • Lymphatic drainage: retropharyngeal node
Endoscopic Anatomy • Medial end forms tubal elevation / torus tubarius • Lymphoid collection over torus is called Gerlach’s tubal tonsil. • Postero-superior to torus is fossa of Rosenmüller.
Physiology • Bony part is always open. • Fibro-cartilaginous part is closed at rest. • Opens on: 1. swallowing 2. yawning 3. sneezing 4. forceful inflation
Physiology • Opens actively by contraction of tensor veli palatini & passively by contraction of levator veli palatini (it releases the tension on tubal cartilage). • Closes by elastic recoil of elastin hinge + deforming force of Ostmann’s fat pad.
Functions 1. Ventilation & maintenance of atmospheric pressure in middle ear for normal hearing 2. Drainage of middle ear secretions into nasopharynx by muco-ciliary clearance, pumping action of Eustachian tube & presence of intra-luminal surface tension
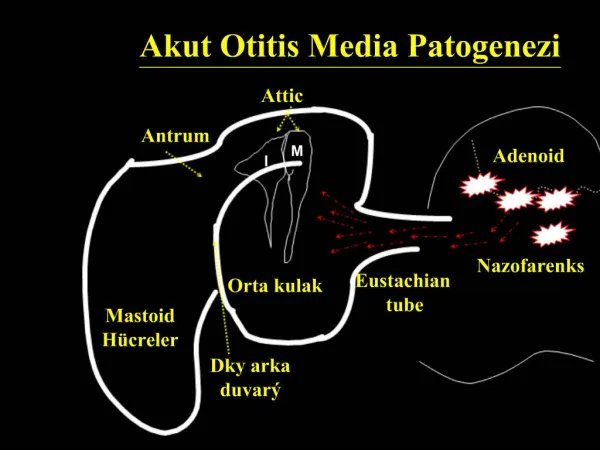
Functions 3. Protection of middle ear from: • Ascending nasopharyngeal secretions due to narrow isthmus & angulation between 2 parts of E.T. at isthmus • Pressure fluctuations • Loud sound coming through pharynx
1. Valsalva Maneuver Forced expiration with mouth & nose closed. Otoscopy shows lateral bulging of Tympanic membrane
2. Frenzel Maneuver • Hands free Valsalva for pilots • Compression of nasopharyngeal air by muscles of tongue • Otoscopy shows lateral bulging of tympanic membrane
3. Toynbee Maneuver • More physiological • Swallowing with mouth & nose closed • Otoscopy shows retraction of tympanic membrane
4. Pneumatic otoscopy & Siegelization • Air pressure is alternately increased & decreased within external auditory canal • Mobility of tympanic membrane is observed • Normal mobility indicates good patency of Eustachian tube
5. Politzerization • Rubber tube attached to a Politzer bag put into one nostril & both nostrils pinched • Patient asked to swallow or repeat “k” • Politzer bag is squeezed simultaneously • Otoscopy shows lateral bulging of ear drum in patent Eustachian tube
6. E.T. catheterization • E.T. catheter passed along nasal floor till it touches posterior wall of naso-pharynx. • Catheter rotated 90° medially & pulled forward till it impinges on posterior nasal septum. • Catheter rotated 180° laterally, & its tip inserted into opening of E.T. • Politzer bag attached to outer end of catheter