Download
1 / 25
270 likes | 688 Views
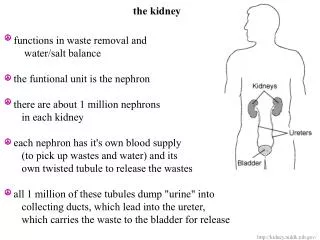
Injuries to the kidney. Introduction. The most common injuries of the urinary system. Although well protected by lumbar muscles, ribs, vertebral bodies and viscera, the kidneys have a great mobility, consequently, parenchymal damage and vascular injuries can easily occur.

E N D
Introduction • The most common injuries of the urinary system. Although well protected by lumbar muscles, ribs, vertebral bodies and viscera, the kidneys have a great mobility, consequently, parenchymal damage and vascular injuries can easily occur. • Trauma is generally caused by falls, road traffic accidents, blows, sporting accidents, stab wounds and gunshot wounds. Spontaneous rupture of the kidney is uncommon, nevertheless most urologists will have seen at least two or three cases during a lifetime of urological practice. • Renal trauma can be classified as either blunt (non penetrating) or penetrating, and both can be divided into two major classifications, the major and minor injuries.
Mode of injury • Blunt renal trauma can be classified according to the severity of injury and the most common is the renal contusion. • Blunt trauma in the region of 12th rib compresses the kidney against the lumbar spine, and the injuries will commonly involve the waist or lower pole of the kidney, where the 12th rib makes its impact. • The kidney can be damaged from a blow in the abdomen anteriorly, just below the rib cage, particularly in road traffic accidents, such as the victim is thrown onto the steering column or some other projecting object. • Abdominal injuries due to seat belts include 11% which involve the urinary tract and half of those are renal.
Mode of injury: penetrating injuries • Penetrating injuries (usually from gunshot or stab wounds) account for 20% of renal traumas in an urban setting. • The damage from a bullet will depend not only on direction, but also on the velocity of the missile. Low-velocity missiles will penetrate all structures in their path. With high-velocity missiles it is necessary to assume that the shock wave will have damaged an area around the track of the missile. • A knife or stiletto stab can readily cut the cortex of the kidney if the weapon is driven more than 3 inches into the victim. Although a peri-renal hematomas usually develops, the patient may not show haematuria unless the weapon has reached the calyces or renal pelvis.
Mode of injury: iatrogenic injuries • There is also the possibility of iatrogenic injuries, that can occur in the passage of a catheter up the ureter (damage of renal pelvis), when a renal biopsy is done or when there is an infection carried indirectly into the renal pelvis.
Classification of Renal Injuries • There are many types of classification, but the principal objective is to determine the extension of the injury and the possible management according to the type of injury. Basically we can divide it in five grades • The grades I and II are classified as minor traumas, and the grades III, IV and V as major traumas:
American Association for the Surgery of Trauma Organ Injury Severity Scale for the Kidney[*] Classification of Renal Injuries
Computed tomographic scan of a right renal stab wound (grade IV), demonstrating extensive urinary extravasation and large retroperitoneal hematoma
Clinical features • Loin or abdominal abrasions or bruising • Loin tenderness • Loss of loin contour • Loin mass • Macroscopic haematuria +/- clot colic • A renal pedicle injury is possible in the absence of haematuria
Investigations • Urine examination: microscopic or gross haematuria • X-ray of the abdomen: fracture of the lower ribs or vertebral body or transverse process • Excretory urograms • USG: controversial • CT scan • Arteriorgraphy
Investigations: excretory urograms • Whatever the type of injury, the investigation for the staging of a renal injury begins with excretory urogram. It permits not only the identification of bone fractures, free intraperitoneal air and displaced bowel but also identify the presence or not of both kidneys, define the renal outlines, the collecting system and the ureters. • It is also indicated when there is the possibility of nephrectomy. This exam shows if the opposite kidney has a normal function, ensuring that the patient will have a normal renal function after nephrectomy.
CT scan • When the excretory urogram does not define well the extent of injury, the patient can be evaluated by a CT scanning or an arteriography. • The CT scanning can distinguish better a major from minor injury, can identify extravasation that were not demonstrated in excretory urogram. It can also distinguish renal laceration and outline an intrarenal hematoma. • Arteriography can be used when there is no CT scan available or when the CT is not a definitive exam, and it may reveal the actual bleeding vessel, show occlusion of the main renal artery or its branches, and also renal lacerations.
Arteriography demonstrating complete occlusion of the left renal artery secondary to thrombus formation
Management • 80% injuries are minor (Class I/II) and can be managed conservatively • Early surgical intervention is required for: • Reno-vascular pedicle injury • Pelviureteric junction disruption • Shock with signs of intraperitoneal or retroperitoneal trauma • Surgery should be performed through a midline incision and transperitoneal approach • Control of the renal pedicle should be obtained before the retroperitoneal haematoma is opened • Surgical priorities are: • Save life - early nephrectomy may be required • Remove devitalised tissue • Preserve renal function - consider partial nephrectomy if possible • Repair and drain collecting system
Renal Reconstruction Technique for partial nephrectomy: A, total renal exposure; B, sharp removal of nonviable tissue; C, hemostasis obtained and collecting system closed; D, defect covered
Technique for renorrhaphy: A, typical injury in midportion of kidney; B, débridement, hemostasis, and collecting system closure; C, approximation of parenchymal margins; D, sutures tied over gelatin sponge bolster
Possible Complications • secondary hemorrhage, usually due to infection (10 to 14 days after trauma); • paralytic ileus (4 to 5 days) as a result of retroperitoneal hematoma; • hypertension as a result of the constricting effect of reorganizing perirenal hematoma; • arterio -venous fistula; • renal failure; • renal atrophy; • hydronephrosis; • chronic pyelonephritis; • renal calculi; • renal artery stenosis.
Case discussion • A 36-year-old forest worker was hit by a falling tree, 3 hours ago. He has pain in the left subscapular region, which is aggravated by taking a deep breath and on anteroposterior and lateral chest compression. He has ecchymoses on anterior and posterior chest and on upper abdominal wall. His abdomen is vaguely tender to palpation in the left upper quadrant (LUQ) and he has left costovertebral angle (CVA) tenderness. The rest of his exam is unremarkable. Chest x-ray is positive for posterior factures of the 8th, 9th and 10th ribs on the left. Abdominal x-ray shows blunting of the left psoas shadow. Abdominal ultrasound is unremarkable. His vital signs are PR: 90/min; BP: 120/80mm of Hg; RR: 18/min. • The laboratory test results are: Hb 15.3 Hematocrit 43% WBC 6,200cmm Urinary sediment: Many erythrocytes; WBC 4-5/ hpf, oxalate crystals.
What is the next most appropriate step in management for this patient? A. Intravenous pyelography B. Diagnostic peritoneal lavage C. CT with contrast D. Lumbar spine X-ray E. Renal angiography