Download
1 / 67
690 likes | 923 Views
Lecture 18. Translational Issues/Biomarkers. JOINT STATEMENT BY PRESIDENT CLINTON AND PRIME MINISTER TONY BLAIR PRESIDENT CLINTON ANNOUNCES THE COMPLETION OF THE FIRST SURVEY OF THE ENTIRE HUMAN GENOME

E N D
Lecture 18 Translational Issues/Biomarkers
JOINT STATEMENT BY PRESIDENT CLINTON AND PRIME MINISTER TONY BLAIR PRESIDENT CLINTON ANNOUNCES THE COMPLETION OF THE FIRST SURVEY OF THE ENTIRE HUMAN GENOME Hails Public and Private Efforts Leading to This Historic Achievement June 26, 2000 Today…. Press release US. Govt.
Specifically… • Now, scientists will be able to use the working draft of the human genome to: • *Alert patients that they are at risk for certain diseases. • *Reliably predict the course of disease. • *Precisely diagnose disease and ensure the most effective treatment is used. • *Develop new treatments at the molecular level. Press release US. Govt.
Analysis of molecular networks via gene expression analysis (gene chips)
However, • Gene expression analysis requires tissue samples directly from the affected site in the affected tissue of the affected person. • Is therefore not suitable for population based screening • Is therefore not suitable for early detection of disease.
Therefore… • If the human genome can be used to: • *Alert patients that they are at risk for certain diseases. • *Reliably predict the course of disease. • *Precisely diagnose disease and ensure the most effective treatment is used. • *Develop new treatments at the molecular level. Then… Most or all of these predictions would be equally well or better solved by proteomics: • Remote sensing of cellular networks by plasma proteome analysis. .
Genomics: • All the possible elements ( genes) are known • All the possible elements are measured in each experiment • No signal detected: element not there Proteomics: • All the possible elements (proteins) are NOT known • All the possible elements are NOT measured in each • experiment • No signal detected: element not there OR element not • detected .
Prinicpal Clinical Proteomic Goals ♦ Identification of proteins or pathways useful as drug targets ♦ Identification of proteins or peptides useful as diagnostics (biomarkers)
Prinicpal Clinical Proteomic Goals ♦ Identification of proteins or pathways useful as drug targets ♦ Identification of proteins or peptides useful as diagnostics (biomarkers)
Biomarker References N. l. Anderson and N. G. Anderson, “The Human Plasma Proteome: History, Character and Diagnostic Prospects”, Mol. Cell. Proteomics 1, 845-867 (2002) N. L. Anderson et al.,”The Human Plasma Proteome:A Nonredundant List Developedby Combination of Four Separate Sources”, Mol. Cell. Proteomics, 3,311-326 (2004) N. L. Anderson, “The Roles of Mulitple Proteomic Platforms in a Pipeline for New Diagnostics”, Mol. Cell. Proteomics, 4,1441-43 (2005)
Protein Biomarkers in Plasma HaveShown Substantial Clinical Value Leigh Anderson, PPI
Is it likely to find tissue specific reporter proteins in plasma by conventional methods?
Blood passes through tissue . . . . . . New proteins are acquired Plasma contains cues regarding the state of a tissue
Clinical endpoint – how a patient feels, functions or survives Surrogate endpoint – a biomarker which can definitively substitute for a clinical benefit endpoint in measurements of drug efficacy Biomarker – a characteristic that is objectively measured and evaluated as an indicator of normal biological processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention A Useful Biomarker Informs risk/benefit ratio when there is a decision to be made Does so in a better/faster/earlier /cheaper way than existing approaches Generally applicable: sample and technology must be available/accessible Has known identity(ies) Definitions
Importantly, biomarkers are not static and can change over time; as such, a single nucleotide polymorphism (SNP) is not a biomarker. This emphasizes the distinction between biomarkers, that can be used to identify disease (or a condition such as inflammation) and to monitor its progress and response to treatment and markers that focus on the evaluation of non-protein material, usually as chips, that is useful for predisposition analyses
Personalized Medicine Biomarkers can be used for: • Patient stratification • Response predication • Unwanted side effects • Monitor disease progression • Monitor positive effects of drug treatments
Biomarkers can be used for: ● Diagnosis • Patient stratification • Response predication • Unwanted side effects • Monitor disease progression • Monitor positive effects of drug • treatments
Types of Proteomic Biomarkers ● Single entities - relative presence or absence compared to normal levels ●Modifications (PTMs)
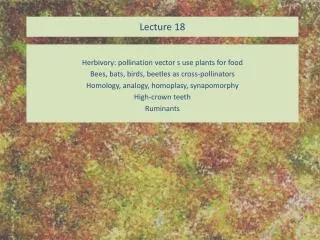
Glycosylation status differs between healthy and malignant tissues Sialic acid and fucose Healthy Malignant
Types of Proteomic Biomarkers ● Single entities - relative presence or absence compared to normal levels ●Modifications (PTMs) ● Multiple entities - identified or unidentified (pattern recognition)
Necessary properties of a biomarker • Address an unmet clinical/diagnostic problem • Be found in a tissue/fluid that can readily be obtained • Amenable to hi-throughput analyses such as an immunoassay • Be readily and reproducibly distinguished from normal levels (which are preferably zero or close to it)
Biomarker Identification - Platform Requirements • High dynamic range and extensive coverage of the proteome • Highly confident and specific protein identifications • Accurate quantification in multiple clinical samples • High throughput capability to handle large numbers of samples Qian et al. MCP 5: 1727-44 (2006)
Sources of Biomarkers • Fluids - plasma, urine, synovial fluid, CSF etc • Tissue - healthy vs diseased
Sources of Biomarkers • Fluids - plasma, urine, synovial fluid, CSF etc • Tissue - healthy vs diseased
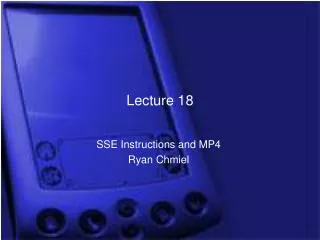
Human Plasma Proteome • Primary clinical specimen • ~15 proteins account for 99% of the mass • Contains classical “plasma proteins” and tissue proteins (as leakage markers) (these represent subsets of proteins from other proteomes) • Huge dynamic range (12 orders of magnitude) • Highly complex due to PTMs, e.g. glycosylation, and splice variants/proteolytic products • Substantive genetic and non-genetic heterogeneity in individual samples • 1175 non-redundant products identified (but this is a moving target) • Only a handful of plasma proteins are currently used in routine clinical diagnosis
Plasma Protein Content • Proteins secreted by solid tissues acting in plasma (largely by liver and intestine) • Immunoglobulins (107 sequencesin an average adult) • “Long distance” receptor ligands (endocrine substances) • “Local” receptor ligands (cytokines and other GFs that leak into plasma) • Temporary passengers (eg lysosomal proteins) • Tissue leakage products (from dead or dying cells) • Aberrant secretions (from tumor or other pathological tissues) • Foreign proteins (from parasites and other infectious organisms)
The Serum Challenge : Significant Dynamic Range Range of LC-MS and Most other methods Target range (From Anderson & Anderson (2002) MCP, 1, 845-67)
Anderson NL and Anderson NG, Mol Cell Proteomics 1, 845-67 (2002)
Approaches for Removing Abundant Proteins of the Plasma Proteome • Gel Filtration • Immunoadsorbents • Affinity reagents • Protein EqualizerTM Technology (Protein MinerTM)
Post-Translational Modifications • Signaling systems that underlie many diseases, particularly cancer, depend on reversible PTMs for propagation. • As such, they offer opportunities for detecting disease states dependent on them • Potential to complement discoveries from other types of biomarker searches • May also be tied to drug target identification
Krueger and Srivastava. Mol Cell Proteomics 2006 5: 1799-1810
Krueger and Srivastava. Mol Cell Proteomics 2006 5: 1799-1810
Population Proteomics • An applied subdiscipline of proteomics investigating human proteins across and within populations to define individual protein diversity. • It probes protein modifications in specific proteins from a large number of individuals, utilizing top-down, targeted affinity mass spectrometry approaches. • The measurements may yield new biomarkers and may also reveal new PTMs
The Proteomics Biomarker Track Record • Few, if any, new biomarkers resulting from proteomic identification, validation and clinical approval are being found • Actual number of new protein targets is declining (proteomics is NOT changing this) • In fact, only a handful of proteins are effective as markers; instead there are whole families of commercial products targeting the same small group W. Zolg, MCP 5: 1720-26 (2006)
Only a handful of new protein diagnostics Introduced in past 15 yrs and current rate is only ~1.5/yr Leigh Anderson, Clin Chem, in press
Why is the record so bad? • Technology not yet able to overcome problems of dynamic range and sample complexity?
At least a 1012 dynamic range Shrink the haystack? Biomarker panel? Biomarker Discovery …..is like finding a needle in a haystack ….may turn out to be as difficult as drug discovery ….may require a panel of markers.
Why is the record so bad? • Technology not yet able to overcome problems of dynamic range and sample complexity? • Bad luck?
Why is the record so bad? • Technology not yet able to overcome problems of dynamic range and sample complexity? • Bad luck? • There are no significant numbers of new markers to find (with any technology)?
But is there a lack of candidates? No… in fact conservative estimates are that thousands of proteins have been identified as potential biomarkers for a wide spectrum of disease conditions So what is the problem?