Download
1 / 41
430 likes | 700 Views
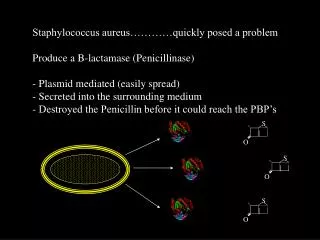
Detection of b -lactamase- mediated resistance. David Livermore Health Protection Agency, Colindale, London. Main b -lactamase threats. Extended-spectrum b -lactamases TEM, SHV & CTX-M types AmpC Derepressed chromosomal e.g Enterobacter Plasmid-mediated in E. coli & Klebsiella

E N D
Detection of b-lactamase-mediated resistance David Livermore Health Protection Agency, Colindale, London
Main b-lactamase threats • Extended-spectrum b-lactamases • TEM, SHV & CTX-M types • AmpC • Derepressed chromosomal e.g Enterobacter • Plasmid-mediated in E. coli & Klebsiella • Carbapenemases • Metallo- & non-metallo-types
ESBL evolution Activity vs 3rd gen cephs TEM-1 1964 Gln39Lys TEM-2 1970 Gln39Lys Glu104Lys Gly238Ser TEM-3 1987
Outcomes: infections with ‘ceph S’ ESBL producers • Prospective study of K. pneumoniae bacteraemia & literature review • 32 evalable patients with ceph ‘S/I’ ESBL producers • 19/32 failed ceph Rx • Bottom line- don’t use cephs vs. ESBL producers, even if they appear susceptible Paterson et al.JCM 2001 39, 2206
Epidemiology of ESBL production • Pre –2000 • Mostly Klebsiella spp. with TEM/SHV • Nosocomial, often ICU / specialist unit • 1998: c. 25% of Klebs from European ICUs ESBL+ • 67% isolates outbreak strains; 33% non-outbreak • Few epidemic strains • - e.g K. pneumoniae K25 SHV-4+ in France • Producers multi-R to quinolones & aminoglycosides
CTX-M b-lactamases • 37 types, 4 clusters • Cefotaximases rather than ceftazidimases • Predominant ESBLs in Argentina since 1990 • 75% of all ESBLs in Buenos Aires • Disseminating rapidly now Asia & Europe
K. georgiana- related K. ascorbata- related CTX-M b-lactamases
CTX-M in the UK • 2000- First producers • K. oxytoca, Leeds, CTX-M-9 • 2001/2- First hospital outbreak • B’ham, 33 patients, K. pneumoniae, CTX-M-25 • 2001/2 • CTX-M-15 in 4 / 922 E. coli from 3 / 28 hospitals Brenwald JAC 2003, 51, 195; Alobwede JAC 2003, 51, 470: Mushtaq JAC 2003 52:528-9
2003 –repeated phone calls • ‘We’ve got these ESBL producers from GP patients. About 20 or 30. Do you want them?’ “The patient hasn’t been in hospital…” ‘Will you I/D it? Our E. coli aren’t resistant like this.’ Is it an Enterobacter?’ “We don’t get bacteria like this from this sort of patient” ‘What do we use?- It’s got an ESBL & it’s trim and cipro resistant. We don’t want to have to admit the patient for i.v. therapy.’
UK, 2003-4: CTX-M-15 E. coli • ARMRL rcvd >500 isolates form >75 UK labs • Mix of hospital and community isolates • Mostly urines; several bacteraemia admissions direct from community • Most age >65; underlying problems, catheterised; hospital contact in past 0-3 years Woodford et al. ECCMID, 2004
PFGE: CTX-M +ve E. coli • 85% similarity = ‘strain’ • 65% isolates - 5 major strains • representatives all serotype O25 • epidemic strain A • 110 isolates, 6 centres • IS26 between blaCTX-M & normal promotor • 4 other major strains, B-E • other isolates • Diverse/small clusters
Geom. mean MICs, (mg/L) CTX-M-15 +ve E. coli Ertapenem & meropenem also active
Spreading CTX-M • CTX-M-2: Israel • CTX-M-3: E. Europe, Far East • CTX-M-5: Latvia, salmonella • CTX-M-9/10-12 Spain • CTX-M-14: China • CTX-M-15: Canada, France, E. Europe (widely) • Russia- ‘CTX-M’s replacing TEM & SHV as the main ESBL types’ ECCMID 2004; ICAAC 2003; Rasmussen & Hoiby 2004 Can J Micro50, 137.
17th July 2004: CTX-M on Fleet St.
Basal in: E. coli & shigellae Inducible in: Enterobacter spp. C. freundii M. morganii Serratia spp. P. aeruginosa 2nd, 3rd gen cephs: Labile, but weak inducers, select derepressed mutants AmpC -lactamases Derepressed Inducible Amt -lactamase [ -lactam]
AmpC -lactamases • Cephalosporins select derepressed mutants from inducible populations • Selection c. 20% in Enterobacter bacteraemia • 30-40% of all Enterobacter and C. freundii now derepressed at first isolation • Resistant to inhibitors; escaping to plasmids
Acquired carbapenemases • IMP & VIM metallo-b-lactamases (Class B) • Scattered reports- Far East; Europe • Mostly in non-fermenters • Class A non-metallo-b-lactamases • KPC small outbreaks in NE USA, Klebsiella & Enterobacter • NMC/IMI in Enterobacter; SME in Serratia: v rare • Class D non-metallo-b-lactamases • Important in Acinetobacter spp.
ESBL Detection: step 1 • Screen Enterobacteriaceae with : • Cefpodoxime- best general ESBL substrate • Cefotaxime & ceftazidime- good substrates for CTX-M & TEM/SHV, respectively Spread of CTX-M into community means screening must be wider than before See http://www.hpa.org.uk
Detection of ESBLs: step 2 • Seek ceph/clav synergy in ceph R isolates • Double disc • Combination disc • Etest See http://www.hpa.org.uk
ESBL detection : combination discs: +ve result, zone enlarged 50% M’Zali et al. 2000, JAC, 45, 881
Zone differences (mm), Klebs & E. colic’pod/clav 10+1 mg - c’pod 10 mg
Etest for ESBLs Cefotaxime Cefotaxime + clavulanate
Etest for ESBLs Cefotaxime Cefotaxime + clavulanate
Pitfalls in ESBL detection • Methods optimised for E. coli & Klebsiella • More difficult with Enterobacter • clavulanate induces AmpC; hides ESBL • Do synergy test (NOT SCREEN) with 4th gen ceph • but how sensitive are these for weak ESBLs?
Bacteria not to test for ESBLs • Acinetobacters • Often S to clavulanate alone • S. maltophilia • +ve result by inhibition of L-2 chromosomal b-lactamase, ubiquitous in the species
AmpC hyperproducing- how to confirm • Resistant to 3rd gen cephs not cefepime • No clavulanate synergy • Cefoxitin R • Enlarged zones to 3rd gen cephs if tests done on agar + 100 mg/L cloxacillin • NOT just ‘because its an Enterobacter’
Double disc antagonism for inducible AmpC Cefoxitin Ceftazidime
AmpC inducibility- when to look • Risk is mutation, not inducibility per se • Best to identify & predict risk from species • Just so ‘No’ • Warn clinicians against cephs for infections due to Enterobacter, C. freundii, Morganella & Serratia
Carbapenem resistance investigations • Enterobacteriaceae • Exceptional – needs ref. lab investigation • Acinetobacter spp. • Exceptional – needs ref lab investigation; PCR for Class D (OXA) b-lactamase genes & MBL • P. aeruginosa • Low level (MIC <32 mg/L) – likely OprD loss • High level (MIC >32 mg/L) likely carbapenemase
Detecting class B enzymes:MBL Etests • imipenem (I) vs. imipenem + EDTA (IPI) • ratio 8 consistent with MBL production • zone distortion consistent with MBL production • sensitivity - good ; specificity - poor
Why false +ves with Etest MBL? • EDTA may permeabilise the outer membrane • Zn++ suppresses OprD in P. aeruginosa, inducing imipenem resistance • ?? lack of zinc may induce OprD. Sensitising bug?? • Zinc inactivates imipenem?2 1Carmen-Conjeho et al., ECCMID, 2003 2 Baxter & Lambert JAC 1997, 39, 838
MICs (mg/L) for E. cloacaewith metallo-b-lactamases Yan et al., JAC 2002, 50, 503
Some common questions 1 • Can I use cephalexin in UTI screens, not cefpodoxime? • No- some strain A CTX-M-15 +ve E. coli appear S • Can I project cefuroxime S/R from cefpodoxime? • No: impermeable E. coli may be c’pod S; c’furox R • I use cefpirome/clav for confirmation with Enterobacter- can I use for all species? • Not proven- not validated vs. weak producers
Some common questions 2 • I can only have one plate per urine. What to test? • C/pod, cipro, trim, nitro & 2 of amp, c/lex & Aug • How do I report cephs for ESBL producers? • Resistant • How do I report b-lactamase inhibitor combs? • Arguable! Probably at face value….
Summary : b-lactamase detection • Exploit indicator cephs • Cefotaxime & ceftazidime OR cefpodoxime • Cefepime/ cefpirome as stable to AmpC; cefoxitin to ESBL • Use ceph / clav synergy tests to confirm ESBL producers • Avoid cephs vs. AmpC inducible Enterobacteriaceae • Use MBL Etests vs carbapenem R isolates, • Be alert to false +ve results • Know patterns; spot the unusual & refer it!