Download
1 / 45
470 likes | 490 Views
Learn about respiratory failure, its types, causes, and management strategies. Explore normal ABG values and distinctions between acute and chronic RF. Understand the pathophysiology and diagnosis of RF.

E N D
Respiratory Failure (RF) Prof. Omer Alamoudi, MD, FRCP, FCCP,FACP
Respiratory Failure (RF) • Normal ABG • Definition • Classification of RF • Distinction between Acute and Chronic RF • Pathophysiologic causes of Acute RF • Diagnosis of RF • Causes • Clinical presentation • Investigations • Management of RF
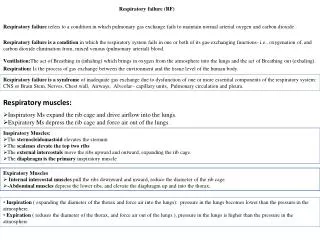
pH 7.35-7.45 PaO2 >70 mmHg PaCO2 35-45 mmHg HCO3 22-28 mmol/l Minute ventilation = Tidal volume X Respiratory rate ↓pH Acidosis ↑pH Alkalosis ↓ PaO2 Hypoxemia ↑PaCO2 Hypercapnia ↓pH+ ↑PaCO2 R. acidosis ↑HCO3 ↑pH+↓PaCO2 R.Alkalosis ↓HCO3 Arterial Blood Gases (ABG) Normal values at sea level
Definitions Clinical conditions in which PaO2 < 60 mmHg while breathing room air or a PaCO2 > 50 mmHg Failure of oxygenation and carbon dioxide elimination Acute and chronic Type 1 or 2 Respiratory Failure (RF)
Classification of RF • Type 1 • Hypoxemic RF ** • PaO2 < 60 mmHg with normal or ↓ PaCO2 • Associated with acute diseases of the lung • Pulmonary edema (Cardiogenic, noncardiogenic (ARDS), pneumonia, pulmonary hemorrhage, and collapse • Type 2 • Hypercapnic RF • PaCO2 > 50 mmHg • Hypoxemia is common • Drug overdose, neuromuscular disease, chest wall deformity, COPD, and Bronchial asthma
Distinction between Acute and Chronic RF • Acute RF • Develops over minutes to hours • ↓ pH quickly to <7.2 • Example; Pneumonia • Chronic RF • Develops over days • ↑ in HCO3 • ↓ pH slightly • Polycythemia, Corpulmonale • Example; COPD
●Hypoventilation ●V/P mismatch ●Shunt ●Diffusion abnormality Pathophysiologic causes of Acute RF
Occurs when ventilation ↓ 4-6 l/min Causes Depression of CNS from drugs Neuromuscular disease of respiratory ms ↑PaCO2 and ↓PaO2 Alveolar –arterial PO2 gradient is normal COPD Pathophysiologic causes of Acute RF1 - Hypoventilation
Pathophysiologic causes of Acute RF ●Hypoventilation ●V/P mismatch ●Shunt ●Diffusion abnormality
Most common cause of hypoxemia Low V/Q ratio, may occur either from Decrease of ventilation 2ry to airway or interstitial lung disease Overperfusion in the presence of normal ventilation e.g. PE Admin. of 100% O2 eliminate hypoxemia Pathophysiologic causes of Acute RF2 -V/Q mismatch
Pathophysiologic causes of Acute RF ●Hypoventilation ●V/P mismatch ●Shunt ●Diffusion abnormality
The deoxygenated blood bypasses the ventilated alveoli and mixes with oxygenated blood → hypoxemia Persistent of hypoxemia despite 100% O2 inhalation Hypercapnia occur when shunt is excessive > 60% Pathophysiologic causes of Acute RF3 -Shunt
Intracardiac Right to left shunt Fallot’s tetralogy Eisenmenger’s syndrome Pulmonary A/V malformation Pneumonia Pulmonary edema Atelectasis/collapse Pulmonary Hge Pulmonary contusion Pathophysiologic causes of Acute RF3 – Causes of Shunt
Pathophysiologic causes of Acute RF ●Hypoventilation ●V/P mismatch ●Shunt ●Diffusion abnormality
Less common Due to abnormality of the alveolar membrane ↓ the number of the alveoli Causes ARDS Fibrotic lung disease Pathophysiologic causes of Acute RF4 -Diffusion abnormality
Hypoxemia Dyspnea, Cyanosis Confusion, somnolence, fits Tachycardia, arrhythmia Tachypnea (good sign) Use of accessory ms Nasal flaring Recession of intercostal ms Polycythemia Pulmonary HTN, Corpulmonale, Rt. HF Hypercapnia ↑Cerebral blood flow, and CSF Pressure Headache Asterixis Papilloedema Warm extremities, collapsing pulse Acidosis (respiratory, and metabolic) ↓pH, ↑ lactic acid Diagnosis of RF1 – Clinical (symptoms, signs)
1 – CNS Depression of the neural drive to breath Brain stem tumors or vascular abnormality Overdose of a narcotic, sedative Myxedema, chronic metabolic alkalosis Acute or chronic hypoventilation and hypercapnia Diagnosis of RF2 – Causes
Diagnosis of RF2 – Causes • 2 - Disorders of peripheral nervous system, Respiratory ms, and Chest wall • Inability to maintain a level of minute ventilation appropriate for the rate of CO2 production • Guillian-Barre syndrome, muscular dystrophy, myasthenia gravis, KS, morbid obesity • Hypoxemia and hypercapnia
Diagnosis of RF2 – Causes • 3 - Abnormities of the airways • Upper airways • Acute epiglotitis • Tracheal tumors • Lower airway • COPD, Asthma, cystic fibrosis • Acute and chronic hypercapnia
Diagnosis of RF2 – Causes • 4 - Abnormities of the alveoli • Diffuse alveolar filling • hypoxemic RF • Cardiogenic and noncardiogenic pulmonary edema • Aspiration pneumonia • Pulmonary hemorrhage • Associate with Intrapulmonary shunt and increase work of breathing
Diagnosis of RF3 – Common causes Hypoxemic RF Hypercapnic RF Chronic bronchitis,emphysema Severe asthma, drug overdose Poisonings, Myasthenia gravis Polyneuropathy, Poliomyelitis Primary ms disorders 1ry alveolar hypoventilation Obesity hypoventilation synd. Pulmonary edema, ARDS Myxedema, head and cervical cord injury Chronic bronchitis, emphysema Pneumonia, pulmonary edema Pulmonary fibrosis Asthma, pneumothorax Pulmonary embolism, Pulmonary hypertension Bronchiectasis, ARDS Fat embolism, KS, Obesity Cyanotic congenital heart disease Granulomatous lung disease
Diagnosis of RF3 - Investigations • ABG • CBC, Hb • Anemia → tissue hypoxemia • Polycythemia → chronic RF • Urea, Creatinine • LFT → clues to RF or its complications • Electrolytes (K, Mg, Ph) → Aggravate RF • ↑ CPK, ↑ Troponin 1 → MI • ↑CPK, normal Troponin 1 → Myositis • TSH → Hypothyroidism
Diagnosis of RF3 - Investigations • Chest x ray → Pulmonary edema → ARDS • Echocardiography → Cardiogenic pulmonary edema → ARDS → PAP, Rt ventricular hypertrophy in CRF ■ PFT- (FEV1/ FVC ratio) Decrease → Airflow obstruction Increase → Restrictive lung disease
Diagnosis of RF3 - Investigations • ECG → cardiac cause of RF → Arrhythmia due to hypoxemia and severe acidosis ■ Right heart catheterization to measure ●Pulmonary capillary wedge pressure (PCWP) ● Normal → ARDS (<18 mmHg) ● Increased → Cardiogenic pulmonary edema
Distinction between Noncardiogenic (ARDS) and Cardiogenic pulmonary edema ARDS Pulmonary edema
ARDS Tachypnea, dyspnea, crackles Aspiration, sepsis 3 to 4 quadrant of alveolar flooding with normal heart size, systolic, diastolic function Decreased compliance Severe hypoxemia refractory to O2 therapy PCWP is normal <18 mm Hg Cardiogenic edema Tachypnea, dyspnea, crackles Lt ventricular dysfunction, valvular disease, IHD Cardiomegaly, vascular redistribution, pleural effusion, perihilar bat-wing distribution of infiltrate Hypoxemia improved on high flow O2 PCWP is High >18 mmHg Distinction between Noncardiogenic (ARDS) and Cardiogenic pulmonary edema
ICU admition 1 -Airway management Endotracheal intubation: Indications Severe Hypoxemia Altered mental status Importance precise O2 delivery to the lungs remove secretion ensures adequate ventilation Management of ARF
2 -Correction of hypoxemia O2 administration via nasal prongs, face mask, intubation and Mechanical ventilation Goal: Adequate O2 delivery to tissues PaO2 = > 60 mmHg Arterial O2 saturation >90% Management of ARF
3- Correction of hypercapnia Control the underlying cause Controlled O2 supply 1 -3 lit/min, titrate according O2 saturation O2 supply to keep the O2 saturation >90% but <93 to avoid inducing hypercapnia COPD-chronic bronchitis, emphysema Management of ARF
Management of ARF Oxyhemoglobin dissociations curve 60mmHg
4 – Mechanical ventilation Indications Persistence hypoxemia despite O2supply Decreased level of consciousness Hypercapnia with severe acidosis (pH< 7.2) Management of ARF
4 - Mechanical ventilation Increase PaO2 Lower PaCO2 Rest respiratory ms (respiratory ms fatigue) Ventilator Assists or controls the patient breathing The lowest FIO2 that produces SaO2 >90% and PO2 >60 mmHg should be given to avoid O2 toxicity Management of ARF
5 -PEEP (positive End-Expiratory pressure Used with mechanical ventilation Increase intrathoracic pressure Keeps the alveoli open Decrease shunting Improve gas exchange Hypoxemic RF (type 1) ARDS Pneumonias Management of ARF
6 - Noninvasive Ventilatory support (IPPV) Mild to moderate RF Patient should have Intact airway, Alert, normal airway protective reflexes Nasal or full face mask Improve oxygenation, Reduce work of breathing Increase cardiac output AECOPD, asthma, CHF Management of ARF
7 - Treatment of the underlying causes After correction of hypoxemia, hemodynamic stability Antibiotics Pneumonia Infection Bronchodilators (COPD, BA) Salbutamol reduce bronchospasm airway resistance Management of ARF
7 - Treatment of the underlying causes Anticholinergics (COPD,BA) Ibratropium bromide inhibit vagal tone relax smooth ms Theophylline (COPD, BA) improve diaphragmatic contraction relax smooth ms Diuretics (pulmonary edema) Frusemide, Metalzone Management of ARF
7 - Treatment of the underlying causes Methyl prednisone (COPD, BA, acute esinophilic pn) Reverse bronchospasm, inflammation Fluids and electrolytes Maintain fluid balance and avoid fluid overload IV nutritional support To restore strength, loss of ms mass Fat, carbohydrate, protein Management of ARF
7 - Treatment of the underlying causes Physiotherapy Chest percussion to loosen secretion Suction of airways Help to drain secretion Maintain alveolar inflation Prevent atelectasis, help lung expansion Management of ARF
Management of ARF • 8 - Weaning from mechanical ventilation • Stable underlying respiratory status • Adequate oxygenation • Intact respiratory drive • Stable cardiovascular status • Patient is a wake, has good nutrition, able to cough and breath deeply
Pulmonary Pulmonary embolism barotrauma pulmonary fibrosis (ARDS) Nosocomial pneumonia Cardiovascular Hypotension, ↓COP Arrhythmia MI, pericarditis GIT Stress ulcer, ileus, diarrhea, hemorrhage Infections Nosocomial infection Pneumonia, UTI, catheter related sepsis Renal ARF (hypoperfusion, nephrotoxic drugs) Poor prognosis Nutritional Malnutrition, diarrhea hypoglycemia, electrolyte disturbances Complications of ARF
Prognosis of ARF • Mortality rate for ARDS → 40% • Younger patient <60 has better survival rate • 75% of patient survive ARDS have impairment of pulmonary function one or more years after recovery • Mortality rate for COPD →10% • Mortality rate increase in the presence of hepatic, cardiovascular, renal, and neurological disease
Suggested text book to read • Davidson’s principle of internal medicine