Download
1 / 19
190 likes | 394 Views
Neuromuscular AND Nervous system. By the end of the lecture the student should Understand the Nervous system Understand brain components Understand cranial nerves Understand sensory system Understand DTR Understand UMN and LMN Understand CVA Understand TBI

E N D
By the end of the lecture the student should Understand the Nervous system Understand brain components Understand cranial nerves Understand sensory system Understand DTR Understand UMN and LMN Understand CVA Understand TBI Understand Nervous System Pathologies Course objectives
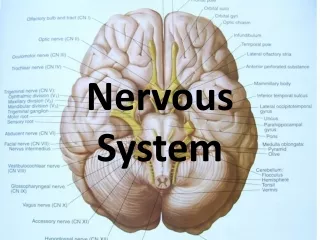
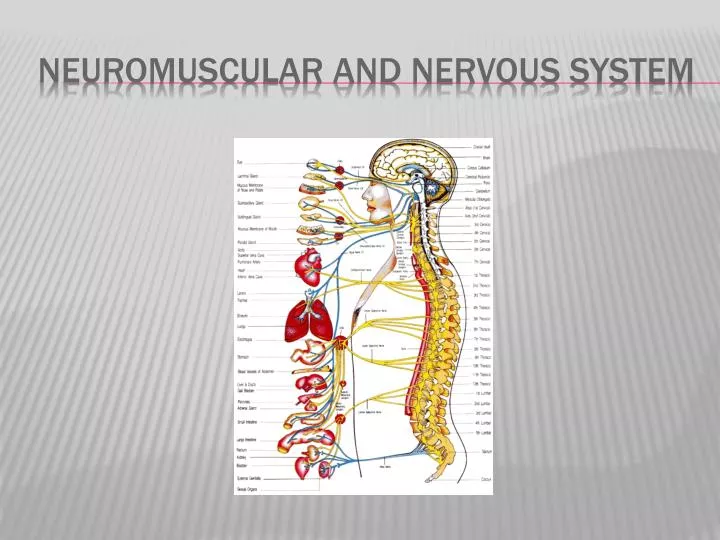
The nervous system is made of the central nervous system (CNS) and the peripheral nervous system (PNS). • The central nervous system is made up of the brain and the spinal cord. • The peripheral nervous system consists of cranial and spinal nerves • The brain controls • The brain is made up of four lobes. • The spinal cord is a made up of neural tracts that conduct information to and from the brain. • Cranial nerves in the peripheral nervous system connect the brain to the head, neck and truck. • Peripheral nerves allow control of muscle groups in the upper and lower extremities and sensory stimulation. • Homeostasis is a state of equilibrium within tissues. • The autonomic nervous system uses neurotransmitters to help conduct nerve signals and turn on/off various cell groups. • Nervous tissue is composed of neurons • A neuron includes a cell body, and organelles usually found in cells. • Dendrites provide receptive information to the neuron and a single axon carries the information away. • Key Terms • Synapse- junction between two neurons • Action potential- threshold at which neurons fire Quick facts Review
Frontal lobe-controls emotions, judgments, controls motor aspects of speech, primary motor cortex for voluntary muscle activation • Parietal lobe-receives fibers with sensory information about touch, proprioception, temperature, and pain from the other side of the body • Temporal lobe-responsible for auditory information, and language comprehension • Occipital lobe- center for visual information • Cerebellum- coordination of muscle function • Brainstem - (midbrain, pons, and medulla)-respiratory and cardiac center, nerve • pathways to the brain • Diencephalon – (thalamus, subthalamus, and hypothalamus) • Thalamus – Integrate and relay sensory information from the face, retina, cochlea, and • taste receptors. (Interprets sensation of touch, pain and temperature). • Hypothalamus • 1. Sleeping Cycle • 2. Controls the autonomic nervous system and the neuroendocrine systems. • 3. Maintains body homeostasis • 4. Thirst Center • 5. Helps regulate body temperature • 6. Helps regulate appetite control • 7. Thirst Center • 8. Control of Hormone secretion Brain
“Oh Once One Takes The Anatomy Final Very Good Vacations Are Heavenly” 1 Nose 2 Eyes 3,4,6 make my eyes due tricks • I-Olfactory-Smell • II-Optic-Vision acuity • III-Oculomotor – Eye function • IV-Trochlear – Eye function • V-Trigeminal – Sensory of the face, chewing • VI-Abducens – Eye function • VII-Facial – Facial expression, wrinkle forehead, taste anterior tongue • VIII-Vestibulocochlear – Auditory acuity, balance and postural responses • IX-Glossopharyngeal – taste on posterior 33% of the scale • X-Vagus – Cardiac, respiratory reflexes • XI-Accessory - Strength of trapezius and Sternocleidomastoid muscles • XII-Hypoglossal – Motor function of the tongue Cranial nerves
Light Touch • Deep Pain • Superficial Pain • Vibration • Proprioception • Kinesthesia • Temperature • Stereognosis • Graphesthesia • Two Point discrimination Sensory System
Facilitation Inhibition Sensory stimulation techniques
DTR elicit a mm contraction when the mm’s tendon is stimulated. Grading • 0+ • 1+ • 2+ • 3+ • 4+ DTR • C5-Bicep • C6-Brachioradialis • C7-Tricep • L4-Patellar Tendon • S1-Achilles Tendon Deep tendon Reflexes
Upper Motor Neuron Lesion • A. Disuse atrophy • B. +Babinski • C. Hypertonia (Spasticity) • D. Weakness/paralysis of movement • E. Hyperreflexia Lower Motor Neuron Lesion • A. True Atrophy • B. Weakness of individual muscles • C. Fibrillations • D. Hyporeflexia Upper vs. lower motor neuron
Anterior cerebral stroke • lower extremity more involved than upper extremity, contralateral hemiparesis and sensory deficits Posterior cerebral stroke • contralateral sensory loss, transient contralateral hemiparesis Middle cerebral artery stroke • upper extremity more involved than the lower extremity, contralateral sensory loss cva
UE • Flexor Synergy • Extensor Synergy LE • Flexor Synergy • Extensor Synergy Aneurysm Precautions • 1. Avoid rectal temperatures • 2. Limit visitors • 3. Avoid Valsalva’s maneuver • 4. Head of bed should be between 30-45 degrees Synergy patterns
No voluntary movement, Initial flaccidity and no tone noted. • Onset of hyperreflexia, synergies and spasticity • Movement in synergy • Decrease in synergy, some voluntary motor control • Progressing improvement with voluntary motor control • Patient has returned to semi-normal state- near normal Brunnstrom Stroke Recovery Stages:
Glascow Coma Scale • +Eye Opening • +Best Motor Response • +Best Verbal Response Level of Consciousness • Coma • Stupor • Obtundity • Delirium • Clouding of Consciousness • Consciousness TBI factors
No response Generalized Response Localized Response Confused-Agitated Confused-Inappropriate Confused-Appropriate Automatic-Appropriate Rancho los amigos
Sympathetic (Fight or Flight): • 1. Dilated pupils • 2. Elevates heart rate and respiratory rate • 3. Sweating • 4. Epinephrine and norepinephrine secreted • 5. Increased blood pressure • 6. Constriction of skin and abdominal arterioles Parasympathetic: • 1. Constricted pupils • 2. Lowers heart rate and respiratory rate • 3. Increased peristalsis • 4. Acetylcholine secreted • 5. Decreases blood pressure • 6. Relaxation of skin and abdominal arterioles Autonomic Nervous System
Valsalva’s maneuver –causes an increase in intrathoracic pressure with an accompanying collapse of the vein of the chest wall. The following may result: • 1. Decreased return of blood to the heart • 2. Slowing of the pulse • 3. Elevated intrathoracic pressure Horner’s Syndrome- A lesion in the brain stem that causes disrupted sympathetic innervation to the face and causes: no sweating, ptosis and papillary constriction. Autonomic Dysreflexia- caused by a lesion in the high thoracic or cervical cord. Severe hypertension, sweating and headaches noted. May occur with a blockage in a urinecatheter. • Signs/Symptoms • 1. Bradycardia • 2. Headache • 3. Increased parasympathetic activity • 4. Excessive perspiration • 5. Excessive sympathetic response • 6. Elevated blood pressure • 7. Stimulation of baroreceptors in aortic arch and caroticd sinus Parkinson’s Disease-a degenerative disease with primary involvement of the basal ganglia; characterized by the following: • Signs/Symptoms • 1. Bradykinesia • 2. Resting tremor • 3. Impaired postural reflexes • 4. Rigidity • 5. Loss of inhibitory dopamine • 6. Mask like affect • 7. Emotional liability Post-polio Syndrome- slowly progressive muscle weakness disease • Sign/Symptoms • 1. Onset of muscle Weakness • 2. Pain/Myalgia • 3. High levels of fatigue Nervous System Pathologies
Multiple Sclerosis–progressive demyelinating disease of the central nervous system • affecting mostly young adults and is chronic. • Cause unknown, most likely viral. • 1. Fluctuating exacerbations • 2. Demyelinating lesions limit neural transmission • 3. Confirmed with lumbar puncture, elevated gamma globulin, CT/MRI, myelogram, • EEG. • 4. Mild to moderate impaired cognition common • 5. Sensory Deficits • 6. Bowel and Bladder Deficits • 7. Spasticity common • 8. Ataxic gait Myasthenia gravis- neuromuscular disease characterized by fatigue of skeletal muscles and muscular weakness. • Signs/Symptoms • 1. Progressive involvement • 2. Decreased muscle membrane acetylcholine receptors • 3. Severe weakness (proximal more than distal muscles) • 4. Facial, ocular and bulbar weakness • 5. Possible life-threatening respiratory muscle weakness • 6. Probable use of anticholinesterase drugs for treatment Guillain-Barre’ Syndrome-polyneuropathy with progressive muscular weakness • Signs/Symptoms • 1. Demyelination of peripheral and cranial nerves • 2. Motor paralysis in an ascending pattern • 3. 3% Mortality – respiratory failure • 4. Autonomic dysfunction-arrhythmias, blood pressure changes, tachycardia Amyotrophic lateral sclerosis (Lou Gehrig’s disease) – degenerative disease that affects anterior horn cells and corticospinal tracts. • Signs/Symptoms • 1. Death typically in 2-5 yrs. • 2. Spasticity, hyperreflexia • 3. Dysarthria, Dysphagia • 4. Autonomic Dysfunction in approximately 1/3 of patients • 5. Cognition is normal Cont. Nervous System Pathologies
Seizures • Epilepsy-recurrent seizures due to excessive and sudden discharge of cerebral cortical neurons. • Tonic-clonic (Grand Mal) –Pt. confused and drowsy about the seizures, 2-5 min generally • Absence seizures (Petit Mal)- Brief, no convulsive contractions, may be up to 100X day • Simple Seizures- no loss of consciousness • Complex Seizures, brief loss of consciousness with psychomotor changes When a patient has a seizure do not use a • tongue blade and allow free movement in a safe environment Meningitis-inflammation of the meninges of the spinal cord and brain caused by bacteria. Signs/Symptoms • 1. Brudzinski’s sign • 2. Kernig’s sign • 3. Stiff/Tight neck • 4. Fever • 5. Confused Cont. Nervous System Pathologies
FSBPT. “2010 NPTE Candidate Handbook.“ 2010. 1-43. Print. • Morrison Media LLC. “NPTAE Secrets.” 2008. 1-171. Print. • Google Images Works cited