Download
1 / 26
260 likes | 525 Views
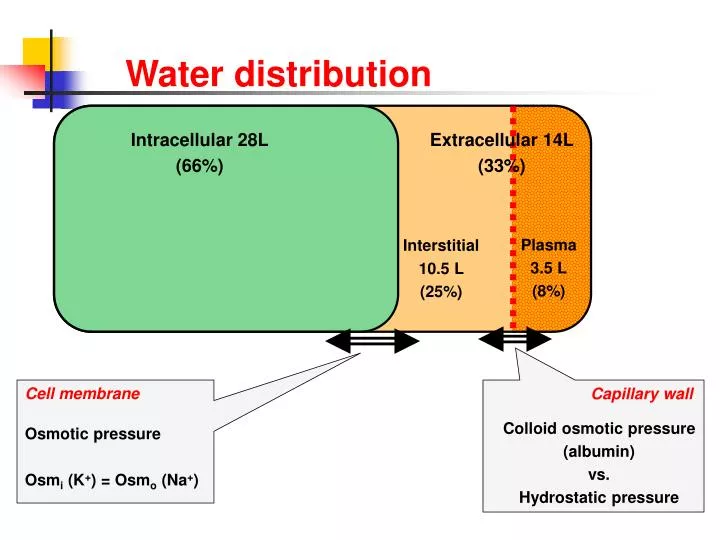
Intracellular 28L (66%). Extracellular 14L (33%). Plasma 3.5 L (8%). Interstitial 10.5 L (25%). Water distribution. Cell membrane Osmotic pressure Osm i (K + ) = Osm o (Na + ). Capillary wall Colloid osmotic pressure (albumin) vs. Hydrostatic pressure. Water Balance. INTAKE.

E N D
Intracellular 28L (66%) Extracellular 14L (33%) Plasma 3.5 L (8%) Interstitial 10.5 L (25%) Water distribution Cell membrane Osmotic pressure Osmi (K+) = Osmo (Na+) Capillary wall Colloid osmotic pressure (albumin) vs. Hydrostatic pressure
Water Balance INTAKE OUTPUT Unregulated: food & social drink Insensible and obligate loss Regulated: thirst AVP modulated water output
Thirst • Hyperosmolar stimulus • hypothalamic osmoreceptors • threshold 1 to 4% above basal • Hypovolaemic stimulus • baroreceptors • threshold 10 - 15% • ? absent in man (inconvenient with postural change!) • Normally inactive as unregulated input is in excess
AVP secretion • Synthesized in hypothalamic supraoptic and paraventricular nuclei • Stored and released from posterior pituitary (> 1 week store!) • Interacts via V2 receptors to insert aquaporin-2 water channels
AVP secretion - stimulation • Osmolar threshold within ‘normal range’ • High ‘gain’ (i.e steep curve and high renal sensitivity) BASAL
AVP secretion - stimulation • Osmotic stimulus high sensitivity • Hypovolaemic stimulus high threshold (>10% depletion)
AVP secretion - stimulation • Osmotic stimulus high sensitivity • Hypovolaemic stimulus high threshold (>10%) • Nausea most powerful known stimulus • Stress e.g. post-operative • Drugs ‘SIADH’
Integration of thirst and AVP • Unregulated water intake supplies water in excess of need • Excess water is excreted • AVP secretion regulates free water clearance • AVP maintains osmolality within narrow limits • This avoids ‘inconvenient’ thirst and water-seeking behaviour • Thirst kicks-in when deficiency reaches harmful levels
Low arterial pressure Low sodium intake Carotid sinus Renin substrate KIDNEY Juxtaglomerular apparatus Low renal Blood flow Renin Angiotensin I (inactive) Thirst Vasoconstriction Angiotensin II Increased perfusion pressure Renal sodium & water retention Aldosterone High K+ Renin-aldosterone system Renin - aldosterone system
Causes of hyponatraemia HYPONATRAEMIA Pseudo- hyponatraemia YES Lipaemia / hyperproteinaemia ? NO Compensatory hyponatraemia Hyperglycaemia ? YES NO Volume depleted Volume expanded Total body water Renal loss Extra-renal loss No oedema Oedema Diuretics Addison’s Vomiting Diarrhoea SIADH Hypothyroid Nephrotic Cirrhosis CCF UNa >20 <10 >20 <10 Rx Normal saline Fluid restriction
Pseudohyponatraemia Aldosterone ADH Na+Na+Na+Na+Na+Na+Na+Na+Na+Na+Na+Na+ Na+Na+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- HCO3- HCO3- HCO3- HCO3- HCO3- HCO3- HCO3- HCO3- Measured sodium concentration 140 mmol/L
Pseudohyponatraemia Aldosterone ADH Na+Na+Na+Na+Na+Na+Na+Na+Na+Na+Na+Na+ Na+Na+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ K+ Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- Cl- HCO3- HCO3- HCO3- HCO3- HCO3- HCO3- HCO3- HCO3- Measured sodium concentration 120 mmol/L Osmolality (solute concentration in water) normal
Case A 17-year old woman was seen in outpatients with a two month history of increasing lethargy and giddiness. She was found to be hyperpigmented and had postural hypotension Serum Ref range Sodium 132 mmol/L 133 – 143 Potassium 5.4 mmol/L 3.6 – 4.6 Urea 8.5 mmol/L 3.0 – 7.0 Creatinine 101 umol/L 55 - 110
Case • A 66-year old man was admitted for investigation of possible bronchogenic carcinoma Serum Ref range Sodium 121 mmol/L 133 – 143 Potassium 4.1 mmol/L 3.6 – 4.6 Urea 4.4 mmol/L 3.0 – 7.0
SIADH - pathogenesis • Inappropriately high AVP levels • Ongoing (unregulated) water intake • Blood volume rises • >10% expansion inhibits aldosterone and triggers natriuresis
Syndrome of Inappropriate ADH Bartter and Schwartz criteria (1967) • hyponatraemia with hypotonicity of plasma • urine osmolality inappropriately high • ongoing renal sodium excretion • absence of oedema or volume depletion • normal renal and adrenal function i.e. Clinically normovolaemic hyponatraemia
Sodium <120 mmol/L Lethargy Anorexia Nausea and vomiting Irritability Headache Muscle weaknes Cramps Sodium <110 mmol/L Drowsiness Confusion Depressed reflexes Extensor plantar responses Seizures Coma Death Syndrome of Inappropriate ADH Symptoms relate to rate of fall as well as severity No oedema because water distributed in both compartments
Neoplasia Carcinoma of lung, pancreas, bladder Leukaemia Thymoma Lymphoma Sarcoma Mesothelioma Causes of SIADH Lung disease • Pneumonia • TB • Pneumothorax • Asthma • IPPV Neurological disorders • Meningitis • Encephalitis • Brain tumour • Subarachnoid haemorrhage • Cerebral and cerebellar atrophy • Guillain-Barré syndrome • Acute intermittent porphyria • Shy-Drager syndrome • Head injury
Causes of SIADH Drugs • Vasopressin • Oxytocin • Vinca alkaloids • Cisplatin • Chlorpropamide • Carbamazepine • Phenothiazines • Thiazides • MAOI’s • SSRI’s • Tricyclics • Nicotine • Ecstacy Miscellaneous • Acute psychosis • Post-operative state • AIDS • Glucocorticoid deficiency • Severe hypothyroidism • Idiopathic
Diagnosis of SIADH • Essential criteria • True plasma hypo-osmolality (<275 mOsm/Kg) • Inappropriate urine osmolality (>~100 mOsm/Kg) • Euvolaemia; no oedema, ascites or intravascular hypovolaemia • Urine sodium not low (>30 mmol/L during normal intake) • Normal renal, adrenal, and thyroid function • Supplemental criteria • Low serum urea and urate • Unable to excrete >80% of water load (20mL/Kg) in 4h and/or failure to achieve urine osmolality <100 mOsm/Kg • No significant rise in serum [Na] after volume expansion but improvement with fluid restriction
Treatment of SIADH • Identification and treatment of underlying cause • Clearance of excess water • not necessary in asymptomatic chronic hyponatraemia • fluid restriction to 500 - 1000 mL/24h • Demeclocycline • 600 to 1,200 mg daily • may take three weeks to reach maximal effect • caution in renal or hepatic insufficiency • Specific V2 receptor antagonists (OPC-31260)
Treatment of SIADH • Hypertonic saline • Only if significantly symptomatic • Calculate sodium required Na+ req. (mmol) = (125 – [Na+]) x 0.6 x body weight (kg) • Also measure and re-infuse urinary sodium output • Rate of increase not usually >0.5 mmol/L/h • ? combine with i.v. furosemide • Stop saline when sodium reaches 120 - 125 mmol/L
Other causes of euvolameic hyponatraemia • Psychogenic hyponatraemia • Massive water intake (20 - 30 L/day) • Urine osmolality <100 mOsm/kg • Beer-drinker’s potomania • High volume low solute drinks impair ability to excrete water • Hypothyroidism • Reset osmostat • Pure glucocorticoid deficiency • Cortisol is required for renal free water excretion
SIADH 1º increase in AVP Inappropriate urine hyperosm. Volume-expansion Suppressed aldosterone Appropriate natriuresis Decreased urea and urate Treatment: fluid restriction CSW Cerebral damage Reduced SNS efferents +/- BNP Inappropriate natriuresis Volume-depletion Volume mediated AVP release Appropriate urine hyperosm. Treatment: Normal saline infusion Cerebral salt wasting
Case 4 • A 53-year old bachelor was brought to the A&E department having been found semi-comatose. He was known to be a heavy drinker of alcohol. On examination he was jaundiced. His abdomen was distended; there was hepatomegaly and evidence of ascites. He had ankle oedema. Serum Ref range Creatinine 84 µmol/L75 – 120 Urea 10.0 mmol/L 3.0 – 7.0 Sodium 111 mmol/L 133 – 143 Potassium 4.9 mmol/L 3.6 – 4.6 Bilirubin 166 µmol/L < 17 Alk phos 175 U/L 21 - 92 ALT 450 U/L 5 – 40 Albumin 24 g/L 35 – 55 Total protein 72 g/L 62 – 80 Globulin 48 g/L 22 - 36