Download
1 / 31
340 likes | 677 Views
Atrial Fibrillation. Steve McGlynn Specialist Principal Pharmacist (Cardiology), Greater Glasgow and Clyde Honorary Clinical Lecture, University of Strathclyde. Some types of arrhythmia. Supraventricular Sinus Nodal Sinus bradycardia Sinus tachycardia Sinus arrhythmia Atrial

E N D
Atrial Fibrillation Steve McGlynn Specialist Principal Pharmacist (Cardiology), Greater Glasgow and Clyde Honorary Clinical Lecture, University of Strathclyde
Some types of arrhythmia • Supraventricular • Sinus Nodal • Sinus bradycardia • Sinus tachycardia • Sinus arrhythmia • Atrial • Atrial tachycardia • Atrial flutter • Atrial fibrillation • AV Nodal • AVNSVT • Heart blocks • Junctional • Ventricular • Escape rhythms • Ventricular tachycardia • Ventricular fibrillation
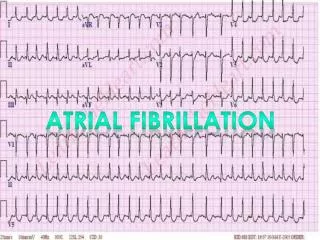
Atrial fibrillation • A heart rhythm disorder (arrhythmia). It usually involves a rapid heart rate, in which the upper heart chambers (atria) are stimulated to contract in a very disorganized and abnormal manner. • A type of supraventricular tachyarrhythmia • The most common arrhythmia
Rheumatic heart disease Coronary heart disease (MI) Hypertension Myopericarditis Hypertrophic cardiomyopathy Cardiac surgery Thyrotoxicosis Infection Alcohol abuse Pulmonary embolism Caffeine Exercise Lone AF Aetiology
1.7 / 1000 patients / year 3 / 1000 patients / year (>60 years) 0.4 - 1% (overall) 2 – 4% (>60 years) >8% (>80 years) Incidence / Prevalence
New / Recent onset < 48 hours Paroxysmal variable duration self terminating Persistent Non-self terminating Cardiovertable Permanent Non-self terminating Non-cardiovertable Classification
Breathlessness / dyspnoea Palpitations Syncope / dizziness Chest discomfort Stroke / TIA 6 x risk of CVA 2 x risk of death 18 x risk of CVA if rheumatic heart disease Irregularly irregular pulse Atrial rate 300-600bpm Ventricular rate depends on degree of AV block 120-160bpm Peripheral rate slower (pulse deficit) Symptoms / Signs
Investigations • Electrocardiogram (ECG) • All patients • May need ambulatory monitoring • Transthoracic echocardiogram (TTE) • Establish baseline • Identify structural heart disease • Risk stratification for anti-thrombotic therapy • Transoesophogeal echocardiography (TOE) • Further valve assessment • If TTE inconclusive / difficult
Investigations • Electrocardiogram (ECG) • All patients • May need ambulatory monitoring • Transthoracic echocardiogram (TTE) • Baseline • Structural heart disease • Risk stratification for anti-thrombotic therapy • Transoesophogeal echocardiography (TOE) • Further valve assessment • TTE inconclusive / difficult
Diagnosis • Based on: • ECG • Presentation • Response to treatment
Treatment objectives • Rhythm / rate control • Stroke prevention
New / Recent onset Cardioversion Rhythm control Paroxysmal Rate control or cardioversion during paroxysm Rhythm control if needed Persistent Cardioversion Rhythm control Peri-cardioversion thromboprophylaxis Permanent Rate control Thromboprophylaxis Treatment strategies
Pharmacological Options • Class Ic Anti-arrhythmics • Flecainide / Propafenone • Rhythm control • May also be pro-arrhythmic • Class II Anti-arrhythmics • Beta-blockers • Mainly rate control • Control rate during exercise and at rest • Generally first choice • Choice depends on co-morbidities
Class III Anti-arryhthmics • Amiodarone / Dronedarone • Mainly rhythm control • May be pro-arrhythmic • Concerns over toxicity • Class IV Anti-arryhthmics • Calcium channel blockers (verapamil / diltiazem only) • Rate control only • Alternative to beta-blockers if no heart failure • Digoxin • Rate control only • Does not control rate during exercise • Third choice unless others contra-indicated
Acute AF Treatment will depend on: • History of AF • Time to presentation (<> 24 hours) • Co-morbidities (CHD, CHF/LVSD etc) • Likelihood of success (History)
Rate Vs. Rhythm control • Rhythm control not feasible or safe • Beta-blocker • Verapamil • Digoxin (CHF) • Rhythm control if possible and safe • DC cardioversion (if possible) • Amiodarone (CHD or CHF/LVSD) • Flecainide (Paroxysmal AF)
Rhythm control* Beta-blocker Class 1c agent or sotalol If CHD - sotalol If LVD: Amiodarone Dronedarone? *May be “Pill in the pocket” Antithrombotic therapy as per risk assessment Aspirin 75-300mg warfarin to INR 2-3 See later Paroxymal AF
Rhythm control Beta blocker No structural heart disease: Class 1c* or sotalol Structural heart disease: amiodarone Rate control As for permanent AF * not if CHD present Antithrombotic therapy as per risk assessment Pre-cardioversion thromboprophylaxis of at least 3 weeks If rate control, as for permanent AF Persistent AF
Beta blocker or Calcium channel blocker and/or Digoxin Amiodarone? Antithrombotic therapy as per risk assessment Aspirin 75-300mg Warfarin to INR 2-3 See later Permanent AF
Stroke Risk Assessment (CHADS2) • C Chronic Heart Failure (1 point) • H Hypertension (1 point) • A Age > 75 years (1 point) • D Diabetes (1 point) • S Stroke, TIA or systemic embolisation (2 points) • Score < 2: low risk, aspirin or anticoagulant • Score ≥ 2: high risk, anticoagulant indicated
Stroke Risk Assessment (CHA2DS2VASc) • Alternative to CHADS2 • C Chronic Heart Failure (1 point) • H Hypertension (1 point) • A Age > 75 years (2 points) • D Diabetes (1 point) • S Stroke, TIA or systemic embolisation (2 points) • V vascular disease (1 point) • A Age 65-74 years (1 point) • Sc Sex category (1 point if female)
Bleeding Risk Assessment(HAS-BLED) • 1 point each for: • Hypertension • Abnormal renal/liver function (1 for each) • Stroke • Bleeding history or predisposition • Labile INR • Elderly (age over 65) • Drugs*/alcohol** concomitantly (1 for each) *Drugs that increase bleeding, e.g. aspirin ** Alcohol excess
Anticoagulants • Warfarin remains standard anticoagulant at present • 3 new oral anticoagulants (unlicensed for AF as of June 2011) • Dabigatran (Direct thrombin inhibitor) • Rivaroxiban (Factor Xa inhibitor) • Apixaban (Factor Xa inhibitor) • Fixed doses • No monitoring • At least as effective as warfarin • Safer than warfarin? • Much more expensive (even allowing for INR costs) • Place in therapy not clear yet
Conclusions • AF is a common condition. • Patients may be unaware of its presence and are therefore at risk of a stroke • Alternative treatment strategies exist to control symptoms • Alternative treatment strategies exist to reduce the risk of stroke • Patient education and choice are central to improving the likelihood of treatment success