Download
1 / 12
120 likes | 399 Views
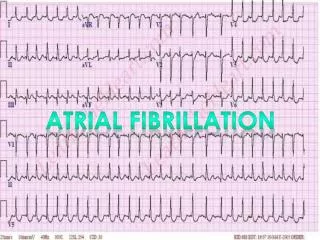
Atrial fibrillation. Key priority ― detection and diagnosis NICE clinical guideline 36, June 2006. Case detection. Assessment. OR. Rate- control. Rhythm- control. Referral. Follow-up. Follow-up. An ECG should be performed in all patients, whether symptomatic or

E N D
Key priority ― detection and diagnosisNICE clinical guideline 36, June 2006 Case detection Assessment OR Rate- control Rhythm- control Referral Follow-up Follow-up An ECG should be performed in all patients, whether symptomatic or not, in whom AF is suspected because an irregular pulse has been detected
Assess for risk of stroke and thromboembolismNICE clinical guideline 36, June 2006 Determine stroke/thromboembolic risk • High risk: • Previous ischaemic stroke/TIA or thromboembolic event • Age >75 with hypertension, diabetes or vascular disease • Clinical evidence of valve disease, heart failure, or impaired left ventricular function on echocardiography • Moderate risk: • Age >65 with no high risk factors • Age <75 with hypertension, diabetes or vascular disease • Low risk: • Age <65 with no moderate or high risk factors
Patients with AF NICE clinical guideline 36, June 2006 Determine stroke/thromboembolic risk Low risk High risk Moderate risk Consider anticoagulation Consider anticoagulation or aspirin Aspirin 75 to 300 mg/day if no contraindications Contraindications to warfarin? YES NO Reassess risk stratification whenever individual risk factors are reviewed Warfarin, target INR = 2.5 (range 2.0 to 3.0)
NICE clinical guideline 36, June 2006. Quick Reference Guide
Treatment for paroxysmal AFNICE clinical guideline 36, June 2006 • Patients with paroxysmal AF can be highly symptomatic • Three main aims of treatment for paroxysmal AF are to: • suppress paroxysms of AF and maintain sinus rhythm • control heart rate during paroxysms of AF • prevent complications • Treatment strategies include out-of-hospital initiation of antiarrhythmic drugs: ‘pill in the pocket’ approach • Patients with paroxysmal AF carry the same risks of stroke and thromboembolism as those with persistent AF
Key priority – choosing the most effective treatmentNICE clinical guideline 36, June 2006 Case detection Assessment OR Rate- control Rhythm- control Referral Follow-up Follow-up • Some patients with • persistent AF will satisfy • criteria for either an initial • rate- or rhythm-control • strategy • Indications for each • option are not mutually • exclusive • Involve the patient in the • treatment decision • Take comorbidities into • account • Antithrombotic therapy • should always be used
Rate control vs. rhythm controlChung MK, et al. Clev Clin J Med 2003;70:567–73
Rate-control strategyNICE clinical guideline 36, June 2006 Try rate-control first for patients with persistent AF: • over 65 • with coronary artery disease • with contraindications to antiarrhythmic drugs • unsuitable for cardioversion • without congestive heart failure
Rhythm-control strategyNICE clinical guideline 36, June 2006 Try rhythm-control first for patients with persistent AF: • who are symptomatic • who are younger • presenting for the first time with lone AF • secondary to a treated/corrected precipitant • with congestive heart failure
Follow-up and referralNICE clinical guideline 36, June 2006 • Follow-up after cardioversion should take place at one month, and the frequency of subsequent reviews should be tailored to the patient • Reassess the need for anticoagulation at each review • Referral for further specialist intervention should be considered in patients: • in whom pharmacological therapy has failed • with lone AF • with ECG evidence of any underlying electrophysiological disorder
Overall summary ― Three steps to AF Heaven • Screen for AF routinely • Checking a person’s pulse is quick and easy • ECG confirmation is needed • Modify stroke risk • Don’t be reticent to use warfarin if the balance of risks and benefits warrants it • Control other risk factors (especially blood pressure) • Choose rate control or rhythm control carefully • Consider patient circumstances • Involve patients in the choice • Specialist referral for rhythm control