Download

1 / 35
430 likes | 1.07k Views
William 2001. Hyaline membrane disease. Hyaline membrane disease Retinopathy of prematurity Respiratory distress in term infants Meconium aspiration. Fetal lungs at birth : ↓ fluid ( expressed or absorbed ) ↑ air ↑ blood Type II pneumocytes surfactant

E N D
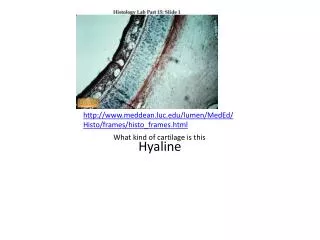
William 2001 Hyaline membrane disease
Hyaline membrane disease • Retinopathy of prematurity • Respiratory distress in term infants • Meconium aspiration
Fetal lungs at birth : • ↓ fluid ( expressed or absorbed ) • ↑ air • ↑ blood Type II pneumocytes surfactant Surfactant ↓ surface tension ↓ surfactant collapse of the alveoli at the end of expiration + hyaline membrane in alveoli and distal bronchioles Hyaline membrane disease
Corticosteroid therapy ↓ HMD HMD ↑ in boys – blacks Preeclampsia and PROM no ↓ HMD Clinical picture: • Tachypnea • Retraction of chest wall • Grunting – flaring Progressive shunting of blood through
nonventilated areas • Hypoxemia • Acidosis ( respiratory – metabolic ) • Hypotension ( systemic – peripheral ) X ray: • Diffuse reticulogranular infiltrate • Air – filled tracheobronchial tree ( air bronchogram )
Other causes of respiratory insufficiency: • Sepsis • Meconium aspiration • Pneumonia • Pneumothorax • Diaphragmatic hernia • Persistent fetal circulation • HF
Common causes of cardiac decompensation in neonates: • PDA • CHD Pathology: Hypotension and hypoxemia Epithelial tissue necrosis Pulmonary HTN + relative R to L shunt
O2 therapy • damage to the lungs & retina • reversal of the shunt Hyaline membrane = • fibrin rich protein • cellular debris • necrotic tissue below it Gross appearance = liver - like
Histologically: • Collapsed alveoli • Some widely dilated alveoli • Vacuolated duct epithelium Treatment: • ICU • If arterial PO2 < 40mmHg give the lowest level sufficient to treat hypoxia and acidosis = PO2 50 – 70 mmHg
Continuous +ve airway pressure (CPAP): - Prevent alveolar collapse↓mortality - Disadvantages: • ↓ VR • Possible barotrauma • Brochopulmonary dysplasia High frequency oscillatory ventilation ± NO for severe pulmonary HTN: Pulmonary VD with no systemic VD
Surfactant: 1st report in 1980 by Fujiwara Helpful in LBW = 500 – 750 gm = 23 – 26 weeks ↓ mortality by 20 – 25% It’s rule in older fetuses debate Types: Biological (animal-human)–synthetic
Complications : • Bronchopulmonary dysplasia • Pulmonary HTN • Retinopathy Bronchopulmonary dysplasia: = O2 toxicity lung disease Alveolar and bronchiolar epithelial damage hypoxia + hypercarbia + O2 dependence peribronchial and interstitial fibrosis P HTN
Prevention: Avoidelective preterm labor: • Estimate GA • Confirm lung maturity Then weigh risks of maternal disease against risks of prematurity Amniocentesis to confirm fetal lung maturity:
1 – Lecithin-to-sphingomyelin ratio: < 34 weeks L/S R = < 2 ≥ 34 weeks L/S R = ≥ 2 RDS ↑ if L/S R = < 2 ↓ if L/S R = ≥ 2 Blood contamination ↑↓ L/S Meconium ↓L/S Tests of lung maturity
Studies on L/S Ratio : • ↓ L/S R is more predictive of the need for ventilatory support # ↓ GA & BW • Some maternal diseases RDS with L/S R ≥ 2 espatially DM • Metabolic and respiratory acidosis in severe DM RDS • Lung maturation not delayed in DM • Delayed lung maturation is associated with poor glucose control
No RDS in blacks if L/S ratio is > 1 ½ 2 – Phosphatidylglycerol: • Enhance surface active properties • Not detected in blood, meconium or vaginal secretions • For more assurance that RDS will not develop • It’s absent does not mean that RDS will develop after delivery • Some do not deliver DM except if it is +ve
3 – TDx– FLM: - Measures surfactant/albumen R - rapid ½ hour - ≥ 50 100% lung maturity - Equal or superior to L/S R, shake and phosphatidylglycerol tests - Some use it as 1st line before L/S 4 - Shake test: 1972
Contamination↑ false –ve results Used as screening test by some 5 – Lumadex – FSI: reliable 6 -- Fluorescent polarization: reliable simple rapid expensive 7 – AF absorbance at 650 - nm wavelength = L/S R
8 - Lamellar body count: Simple – rapid – accurate ≥ 35000/mL = 100% lung mature 9 - Dipalmitoylphosphatidylcholine ( DPPC test ): sensitivity = 100% specificity = 96%
< 1950 = largest single cause of blindness > 1950 = ↓ due to avoiding ↑ O2 therapy - The retina vascularizes centrifugally from the optic nerve starting at the 4th month until after birth . During this period it is easily damaged - ↑ O2 mostly damage the temporal portion of the retina Retinopathy of prematurity
- ↑ O2 severe VC endothelial damage and vessel obliteration hypoxia - ↓ O2 hypoxia neovascularization Hg and proteinaceous material adhesions retinal detachment Prevention: - ↓ O2 to 40% of the inhaled air ( may not be sufficient for very immature fetus ) - Large dose of vit E ( controversial )
Much less frequent Causes: • Sepsis • Meconium aspiration • Intrauterine pneumonia • Persistent pulmonary HTN • Pulmonary Hg Sepsis septicemia mostly due to group - B streptococcus disease Respiratory distress in the term infant
Meconium is usually associated with: • Oligohydramnios • Uteroplacental insufficiency • Fetal distress Persistent pulmonary HTN may follow: • Elective CS • Premature closure of ductus arteriosus
Treatment: Similar to hyaline membrane disease: High frequency oscillatory ventilation + nitric oxide inhalation in severe pulmonary HTN pulmonary VD with no systemic VD ↓ fetal death ↓ need for extracorporeal membrane oxygenation ( ECMO ) But not useful < 34 weeks
Severe pulmonary disease characterized by: Chemical pneumonitis Mechanical obstruction Resulting from: Peripartum inhalation of meconium - stained AF inflammation + hypoxia Free fatty acids remove the surfactant In severe cases pulmonary HTN death or long – term neurological sequelae Meconium aspiration
= % 20 of pregnancies at term In the past MA = fetal distress Now = normal GIT maturation or vagalstimulation by UCcompression But still considered a marker of: adverse perinataloutcome In healthy fetuses + normal AFV cleared Not cleared mostly in thick meconium with: Postterm - FGR
Risk factors: • ↓ AFV • Cord compression • Uteroplacentalinsufficiancy MA ↑ in: • Thick meconium • Abnormal FHR Transient episodes of cord compression may MA in cases of oligohydramnios
MA can not be predicted: - = 20% of normal pregnancies - CS for meconium and abnormal FHR no alteration of % of meconium beneath the cords - Aggressive peripartum airway management did not prevent fetal death
Prevention: Carson 1976 - Oropharyngeal suction of the infant before delivery of the chest - Laryngoscope visualization: If meconium is visualized additional suctioning of the trachea
Studies: - This procedure 2.1% MA = still occur = not caused by delivery - Routine tracheal suction of nondepressed infants with meconium stained AF ↑ morbidity # no suction - MA is caused by chronic antenatal insult abnormal muscularizationof interacinar arteries - MAin baboon model no deathor long – term neurological sequence
- MA is caused by chronic fetal asphyxia pathological changes: • Pulmonary vascular damage • Persistent fetal circulation • Pulmonary HTN - Markers of acute asphyxia are not ↑: pH - lactates - hypoxanthine - 1 Marker of chronic asphyxia is↑: erythropoietin
Amnioinfusion: Used toreliefvariable decelerations during labor: • ↓ VD& cord compression • ↓ MA & meconium below the cords • ↓ Operative delivery • Neonatal acidosis Useful for healthy fetus with thick meconium Not useful for chronic asphyxia
Management of MA: - Suction before delivery of the shouldersby: • Suction bulb • DeLeetrapconnected to wall suction and not suctioned by mouth Study: - Both are equally efficacious - Carful suction 5% MA in moderate to thick meconium
- If the infantis depressed or + thick particulate meconium: Suction under visualization Intubation + tracheal suction Stomach suction - In thin meconium tracheal suction is controversial - Efficacy is unknown skillful suction carry little risk of harm