Download
1 / 29
300 likes | 742 Views
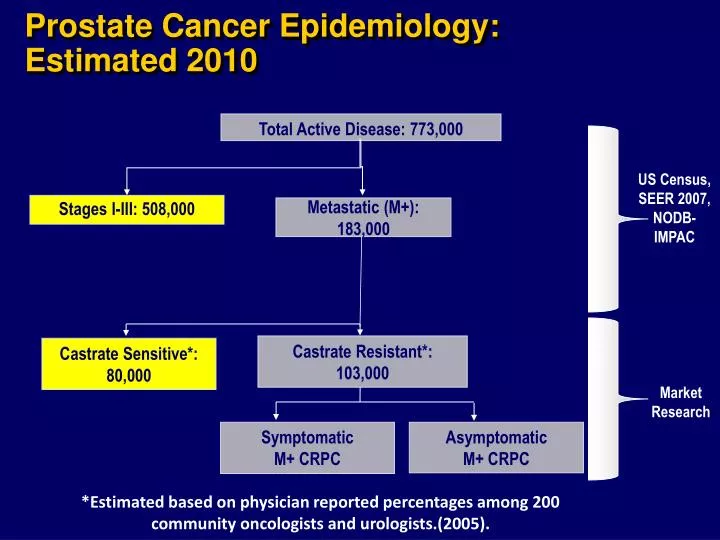
Prostate Cancer Epidemiology: Estimated 2010. Total Active Disease: 773,000. US Census, SEER 2007, NODB-IMPAC. Stages I-III: 508,000. Metastatic (M+): 183,000. Castrate Resistant*: 103,000. Castrate Sensitive*: 80,000. Market Research. Symptomatic M+ CRPC. Asymptomatic M+ CRPC.

E N D
Prostate Cancer Epidemiology: Estimated 2010 Total Active Disease: 773,000 US Census,SEER 2007, NODB-IMPAC Stages I-III: 508,000 Metastatic (M+):183,000 Castrate Resistant*: 103,000 Castrate Sensitive*: 80,000 Market Research SymptomaticM+ CRPC Asymptomatic M+ CRPC *Estimated based on physician reported percentages among 200 community oncologists and urologists.(2005).
Life After Traditional Androgen Deprivation Failure • Other Hormonal Therapy • Chemo Therapy • Immunotherapy
Rationale For Immunotherapy Cancer Cellular dysfunction Resistance to or escape from host defenses Active immunotherapy Suitable target antigen Effective presentation of antigen Mobilization of immune cascade
Antigen Presenting Cells (APCs) Dendritic cells (DCs) are antigen-presenting cells that process and present MHC-peptide complexes to activate a T-lymphocyte response
T-cell CD8CD4 CD154 CTLA4 CD11/CD18 CD28 TCR Peptide MHC class IMHC class II CD54 CD80CD86 CD40 Dendritic cell
sipuleucel-T (Provenge®) sipuleucel-T is an autologous active cellular immunotherapy that activates the immune system against prostate cancer
Sipuleucel-T: Patient-Specific Therapy Day 1 Leukapheresis Day 2-3 sipuleucel-T is manufactured Day 3-4 Patient is infused Apheresis Center Dendreon Doctor’s Office COMPLETE COURSE OF THERAPY: Weeks 0, 2, 4
Primary Endpoint (Trial 9901)Time to Disease Progression Study 1 Percent without Progression Weeks
Secondary Endpoint - SurvivalClinically Significant and Statistically Persuasive Overall Survival Benefit Median benefit4.5 months 34% 11%
Vote of FDA Expert Panel 17 – 0 for safety 13 – 4 for substantial evidence of efficacy FDA Requires More Data (<2% Event)
Randomized Phase 3 IMPACT Trial(IMmunotherapy Prostate AdenoCarcinoma Treatment) P R O G R E S S I O N S U R V I V A L Treated at Physician discretion Sipuleucel-T Q 2 weeks x 3 Asymptomatic or Minimally Symptomatic Metastatic Castrate Resistant Prostate Cancer (N=512) 2:1 Treated at Physician discretion and/or Salvage Protocol Placebo Q 2 weeks x 3 Primary endpoint: Overall Survival Secondary endpoint: Time to Objective Disease Progression
Eligibility Criteria • Metastatic castrate resistant prostate cancer • Life expectancy of at least 6 months • Serum PSA ≥ 5.0 ng/mL • Castrate level of testosterone (< 50 ng/dL) achieved via medical or surgical castration • Adequate hematologic, renal, and liver function • Negative serology for HIV 1 & 2, HTLV-1, and Hepatitis B & C
IMPACT Overall Survival: Primary EndpointIntent-to-Treat Population P = 0.032 (Cox model) HR = 0.775 [95% CI: 0.614, 0.979] Median Survival Benefit = 4.1 Mos.
Most Common Adverse Events (≥ 5%) Higher Rate in Sipuleucel-T (p ≤ 0.05)
Serious Adverse Events*Safety Population *Occurring in ≥ 4 patients.
Consistency Across Phase 3 Studies • *Unadjusted Cox model & log rank • **Cox model adjusted for PSA and LDH
Summary • First active immunotherapy to demonstrate improvement in overall survival for cancer • Highly favorable benefit to risk profile • Short duration of therapy • Potential to create new paradigm in treatment of metastatic, castrate resistant prostate cancer
Time to Objective Disease Progression • Secondary endpoint • Result • Independent radiologic review • HR=0.951 (95% CI: 0.77,1.17); P=0.628 (log rank) • Consistent with other trials in advanced prostate cancer • Difficult endpoint to measure reliably and doesn’t correlate with overall survival
PSA-TRICom Randomized Phase II Study P R O G R E S S I O N S U R V I V A L Treated at physician discretion PROSTVAC-VF Tricom + GM Asymptomatic or Minimally Symptomatic Metastatic Castrate Resistant Prostate Cancer (N=125) 2:1 Treated at physician discretion and/or Salvage Protocol Empty Vector + placebo Primary endpoint: Progression Free Survival Secondary endpoint: Overall Survival
Background-The Development of PROSTVAC-VF-Tricom • Vaccinia • Potent immunological priming agent • Derived from wild-type Wyeth strain (used in millions of immunizations) • Fowlpox • Minimally/non-cross-reactive with vaccinia • Enables boosting • Slightly altered PSA transgene • Tricom • Lymphocyte function-associated antigen LFA-3 (CD58) • Intercellular adhesion molecule ICAM-1 (CD54) • Costimulatory molecule for the T-cell receptor B7.1 (CD80)
Prime Boosts PROSTVAC-PSA-Tricom Vaccinia-PSA-Tricom Fowlpox-PSA-Tricom
Conclusions • Poxviral-based immunotherapy is feasible and safe • Primary endpoint of prolonged PFS was not met • Secondary endpoint of prolonged median OS • 8.5 month difference in OS, HR 0.56 (95% CI 0.37-0.85) with p=0.0061 • Baseline characteristics of patients in both arms similar • Need to validate these findings in large Phase III study with survival endpoint