Download
1 / 61
620 likes | 672 Views
Learn the core task of assisting with individual therapy, including purpose, interpreter usage, and alerts in patient care. Understand equipment preparation and environmental considerations for therapy sessions to achieve the best patient outcomes.

E N D
ALLIED HEALTH ASSISTANTCORE COMPETENCY: INDIVIDUAL THERAPY LEARNING PACKAGE
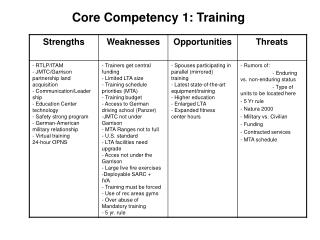
INTRODUCTION A core task for Allied Health Assistants (AHAs) is to assist with delivering individual therapy to patients according to the specific care plan that has been prescribed by an Allied Health Professional (AHP). There are a range of skills required to deliver this therapy in a way which will achieve the best outcome for the patient.
AHA SCOPE OF PRACTICE An individual AHA’s Scope of Practice specifies the roles and responsibilities that the AHA is educated, authorised and competent to perform. Key elements of this are: • Grading of the position • Position description • Duty statement • Qualifications • Level of experience • Competency
PLAN AND PREPARE Competency areas: • Describe purpose of the individual therapy session 2. Identify when an interpreter is required 3. Identify alerts in patient file or handover that may impact on therapy session
1. Purpose It is important that the AHA is clear on what the purpose and outcome of the therapy session will be, to ensure that: • Appropriate activities are selected • Activities are targeted to achieve the goals • The AHA can explain the purpose of the session to the patient • The AHA can give appropriate instructions and feedback to the patient If the AHA is not clear on the purpose/outcome of the session, the AHA should ask the AHP to explain it.
Example The AHA is preparing for a therapy session with a four year old child, Jarryd, where the purpose of the session is to help Jarryd say“ f” sounds correctly. The speech pathologist, Amanda, has asked the AHA to see Jarryd today to help him practise. Jarryd already knows how to say“ f” and can do it correctly when he copies someone, but he often forgets at other times. Amanda has explained that she wants the AHA to remind Jarryd to use his “ f” sound. Amanda explains to the AHA how to do this and what she should do if Jarryd has difficulty. It is important for the AHA to know that the purpose is for Jarryd to remember to use the sound by himself, not just be shown how to do it and to copy. If the AHA did not know this, she may work on the incorrect goal and slow down Jarryd’s progress. To explain this in the therapy session to Jarryd’s carer, the AHA could say: “Today we will be practising Jarryd’s “f” sound. Because he can already make the sound correctly when he copies us, we want him to start learning to do it by himself. So today we will just remind him how to say it.”
2. Interpreter It is important to ensure that an interpreter is always used when: • The AHP advises that an interpreter should be used • The alert in the medical file indicates an interpreter is required • The patient reports difficulty speaking and understanding English and that they would like an interpreter If the AHA is unsure if an interpreter is needed, check with supervising AHP or ask the patient.
Example Mrs G is from a Croatian background and has limited conversational English. The AHP advises the AHA that Mrs G will need an interpreter for her therapy session. The AHA had already checked Mrs G’s medical record and saw the “interpreter required” alert. This was consistent with the information provided by the AHP. The AHA books an interpreter for the therapy session according to organisational processes.
3. Identify Alerts The AHP should inform the AHA of any relevant alerts regarding a patient. These may include: • Recent changes in health status • Falls risk/mobility status • Infection control precautions • Aggression • Need for interpreter • Modified diet • Protective issues/orders
3. Identify Alerts (cont.) The AHA should know where to look in the file to find out more detail about these alerts if required. The AHA should always speak to the AHP if there are any questions about these alerts, what they mean, how to manage them and how to minimize risk.
EQUIPMENT AND ENVIRONMENT Competency areas: • Physically prepare treatment environment for therapy session • Clean equipment and materials according to manufacturer’s and organisational requirements • Store equipment and materials according to manufacturer’s and organisational protocols • Report equipment faults to appropriate person • State correct ordering procedures for equipment items • Describe process to maintain and monitor stock levels of consumables
1. Physically prepare treatment environment Before the AHA begins a therapy session, it is important to make sure that the therapy area is suitable to address the goals of the session. Issues to consider are: • Room bookings • Equipment / resources needed • AHA knowledge of equipment use (refer to AHA Core Competency – Equipment and Environment)
Example The AHA is preparing for Mrs G’s therapy session as directed by the AHP to meet the goals of the session. The following will be required: • a bed for exercises • an area to practice walking with her walking stick, which is not cluttered with other equipment or not in a high traffic area which might be unsafe • a set of steps • an exercise bike The steps may be in the physiotherapy gym area but someone may have left a box on the second step and have forgotten to remove it. The AHA would check the steps (and other therapy areas) prior to using them to ensure that the area is clear and that there are no items around to cause a tripping hazard. The AHA needs to be aware of how to set up the exercise bike correctly to use it safely.
2 & 3: Cleaning Equipment All equipment needs to be clean for patient use. The AHA should check the cleanliness of equipment before and after all therapy sessions. Equipment should be cleaned and stored in accordance with manufacturer’s and organisational requirements (e.g. may use detergent wipes or not use harsh solvents). This may also include a cleaning schedule at periodic intervals. Organisational infection control policies and procedures may need to be taken in to account.
4. Report equipment faults If there is a specific safety issue with a piece of equipment this should be reported immediately to the appropriate person. This may be the AHP or another designated person.
Example The AHA sees that the exercise bike seat will not adjust - the pins that lock the seat in place are not functioning. The AHA needs to follow organisational policy. This may include: • placing a clear notice on the bike stating that it is not fit to use • removing it from the gym area if it is possible to do so (may be too bulky to move and prove to be an OH&S risk) • discussing the issue with the supervising AHP • organising repair of the bike by a suitably qualified person (may be under manufacturer warranty, or manufacturer may only have approved repairers). This may be done in consultation with the AHP • overseeing this process from the initial request for repair to the re-introduction of the equipment to safe use.
5. Ordering Equipment Consumable items may be used during therapy sessions. Examples of these may include: • theraband exercise tubing for physiotherapists • splinting materials for occupational therapists • specific dietary handouts for dietitians • communication boards for speech pathologists • dressings for podiatrists AHAs commonly have responsibility for ordering consumable items. The AHP will advise the AHA regarding ordering responsibilities. The AHA needs to be familiar with organisational ordering procedures and processes.
6. Maintain and monitor stock levels The AHA may be required to maintain the stock levels of consumables. There will be specific suppliers that will be used at various workplaces. Maintenance of the stock levels may include: • Ensuring suitable storage environment (e.g. some items may need to be stored out of direct sunlight) • Knowing the required levels and keeping a register • Checking the stock levels within an agreed time frame (e.g. weekly/ monthly) • Keeping a current list of supplier details and the time required for delivery • Submitting order requests
6. Maintain and monitor stock levels(cont.) • Organising for delivery • Photocopying • Stock management, such as: • stock rotation to ensure the oldest items are accessed first • checking use by dates • disposing of out of date items as per organisational protocols. • If the items are to be purchased by patients, ensuring the prices are accurate and listed in the agreed area Clear specification of which stock is required to be maintained and monitored should be clarified with the supervising AHP.
CONDUCT INDIVIDUAL THERAPY Competency areas: • Introduce self to patient, including name, role, and wearing ID badge in a clearly visible place • Verbally communicate at a level which is judged to be appropriate to the patient’s level of language, cognition, knowledge of their own condition, and cultural factors • Explain therapy activities to the patient • Determine the patient’s understanding of therapy • Obtain patient’s consent prior to performing activities • Carry out therapy according to instructions from AHP
CONDUCT INDIVIDUAL THERAPY(cont.) • Report at least 3 factors which could indicate the need to cease or modify the therapy • Cease or modify therapy as appropriate • Describe an appropriate prompt to use in therapy • Demonstrate appropriate use of a prompt • Provide constructive feedback to the patient about performance • Respond appropriately to questions from patient within AHA knowledge and skill level and refer to AHP where appropriate • Seek support from the AHP if difficulties arise during therapy • Run sessions to time
1. Introduction Upon commencing work with a patient, it is important to establish rapport with the patient and any family members or carers who may also be in attendance. At the first meeting, it is expected that the AHA member will: • warmly greet the patient by name • state their own name and their role (position they hold at the organisation) • Wear their staff ID badge and nametag in a clearly visible place Example: “Hello Mary. My name is Sue. I am an allied health assistant, which is someone who helps the therapists deliver services to patients. I am here to see you today with your physiotherapist, Stephen.”
2. Communication Patients present from a variety of cultural and educational backgrounds, with a range of skills and knowledge. Some patients may have difficulty hearing, understanding language, expressing themselves, have unclear speech or difficulty maintaining attention. AHAs must take into consideration all of these factors when communicating with patients, to ensure that the patient feels comfortable and understands what is being said. Effective communication is essential to gain the most from each session.
2. Communication (cont.) Factors to be considered may include: • The age of the patient. For example, when communicating with a child, it is important to be down at the child’s level, use fun, simple words, and present with a positive and happy manner to encourage the child to engage. • Sensory impairments, such as hearing or vision loss. Consider if the patient wears glasses, uses a hearing aid, or whether there is a need to speak a little louder. • Patients from non-English speaking backgrounds. Is an interpreter required? Refer to “Interpreter” in PLAN/PREPARE • Impairment due to injury or illness. Communication changes can occur in patients when they have had a brain injury (such as a stroke or a head injury), or they have a mental illness or dementia.
2. Communication (cont.) The AHA must ensure that the language used is at an appropriate level for the patient to understand. For some patients this may include: • Avoiding technical and medical language • Being clear and specific with information/instructions • Avoid giving large amounts of information at one time
2. Communication (cont.) The AHA should always be monitoring the patient’s responses and looking for signs that may indicate a need for the AHA to change communication style, such as the patient: • not following instructions correctly • giving inappropriate responses to questions • appearing disinterested or losing focus • frequently asking for or requiring repetition of information
2. Communication (cont.) Ways that an AHA can modify their communication style to adapt to the patient’s needs include: • Simplifying vocabulary • Shortening sentences • Repeating information • Allowing patient time to process and respond to information • Breaking instructions into individual steps • Calling patient’s name first to gain attention • Establishing eye contact when speaking • Asking the patient if they have understood • Using gestures to support speech • Using an interpreter • Seeking advice of family member
Example An AHA is working with Mr B practising independence with showering. The AHA says: “Step into the shower with your right foot. Hold on as you step in..” Mr B proceeds to reach forward holding the shower screen, which could not support his weight. The AHA had anticipated that Mr B would hold on to the shower rail. The AHA observes that Mr B does not follow the instruction as the AHA had anticipated. The AHA realises that the instruction was not sufficiently specific to ensure Mr B understood what was required. The AHA repeats the instruction as: “Let’s practise that again. This time hold onto the shower rail.”
Example An AHA is working with Ms A, who is recovering from a stroke. The therapy session is aiming to work on balance retraining. The AHA says: “Stand between the rails and keep both feet shoulder width apart and heels on the ground. Don’t move your arms and remember to keep your eyes open all the time and don’t move your head.” Ms A stands up between the rails looking blank and asks “What am I supposed to do next?” The AHA realises that the instruction was too long and complex and that Ms A did not understand. She repeats the instruction by breaking it down into steps: “Put your feet like mine” (the AHA waits until Ms A does this), then continues: “Arms by your side” etc.
2. Communication (cont.) The AHP may inform the AHA of specific communication factors to consider during the therapy session with particular patients. If the AHA is having difficulties communicating with a patient, the AHA should discuss this with the AHP to identify strategies to use.
3. Explain therapy activities Before commencing therapy, it is important that the patient has a clear understanding of the nature of the therapy. The purpose of the activity should be described as well as explaining how this will assist the patient. Providing patients with all appropriate information about the therapy allows patients to give consent (see Patient Consent).
Example “Stephen, the physiotherapist, asked me to come today so I can work to help you with your exercises. Stephen has put together a program of exercises to help strengthen your legs. These exercises will help you manage climbing up your stairs at home.” “Emma, the speech pathologist, asked me to come today to help you with your speech exercises. Emma has given me some exercises we can practice together to help you pronounce some sounds, which will make it easier for your family to understand you when you are speaking.”
4. Patient Understanding After the therapy has been explained, the AHA should confirm that the patient understands what they have been told and check if the patient has any questions. Patient understanding is necessary for the patient to consent to therapy (see “Patient Consent”).
Example “Do you understand what we will be doing today? Do you have any questions?” If the patient has not understood, repeat the information trying to use simpler language. Try breaking the information into small steps to avoid giving too much information at a time. The AHA should answer any questions that the patient may have, provided they are within their scope of practice.
5. Patient Consent It is important to ensure that the patient agrees to the goals and activities of the session. If the patient has any concerns about the activities, the AHA should: • re- explain to make sure the patient has understood • ask the patient to explain their concerns, and discuss with the patient where this is within the AHA scope of practice • refer any other concerns to the AHP. This could include: • asking the AHP to come into the session to talk to the patient • checking information with the AHP and reporting it back to the patient • rescheduling the session in consultation with the AHP.
Example “Are you happy to do the activities that we discussed?”
6. Carry out the therapy program The AHP will have a therapy plan for the AHA to follow. The AHA is required to complete the therapy according as outlined by the AHP (Refer to AHA Core Competency Communication of Patient Information). The AHA must have a thorough understanding of this plan before commencing the session with the patient. The AHA should raise any questions about what is required with the AHP prior to the session.
6. Carry out the therapy program(cont.) The AHA should have a good understanding of: • relevant information about the specific patient, as determined by the AHP (e.g. relevant medical history, family circumstance, need for interpreter etc.) • the goals of the session • required equipment will be needed and how it should be set up • required patient handouts/brochures • instructions to give the patient (continued on next page)
6. Carry out the therapy program(cont.) • amount of support/models/prompts to provide to the patient – if the patient is starting a new activity, they will likely need more support. If the patient has been working on an activity before, the AHP may be aiming for them to gain independence and be less reliant on support (refer also to “Prompts” below). • how patient performance will be recorded • when and how the activities should be modified • length of the therapy session • how/when the AHP will be involved • plans for after this session – e.g.: should the patient be re-booked to attend again, who will see the patient next time
8. Cease or modify therapy It is important to continually monitor the patient and their performance during therapy activities. The patient may show signs that the activities need to be made easier or stopped, such as: • Patient disengages from activity • Patient distress • Significant pain • Shortness of breath • Safety risk • Patient request to discontinue or reports activity is too difficult • Patient taking significantly longer than expected to complete task • Patient demonstrates challenging behaviours The AHA should seek advice from the AHP regarding actions to take in these situations.
Example Mrs. G arrived for her therapy session and reported no new issues. The AHA noticed that Mrs. G had a large bruise on her right arm when she lay on the bed to begin the exercise session. Mrs. G had not mentioned anything to the AHA at the commencement of the session when the AHA introduced herself and when asked how she had been since the last session. The AHA also noticed that Mrs. G appeared a little confused. The AHA then said to Mrs. G that she had seen the bruise on her arm. Mrs. G replied: “Oh yes I blacked out yesterday in the backyard but I am all good now. I didn’t think it was relevant. I am coming here for my leg not my arm. I have had a few dizzy spells over the last few days and have been meaning to see the doctor. I will get around to it in the next few days”. At this point the AHA ensured Mrs. G was safely lying on the bed and that there was a staff member in the gym who would watch Mrs. G. The AHA then advised Mrs. G to rest on the bed and that she would go and contact the AHP. The AHA informs the AHP of the issues Mrs. G has raised and states that she believes the therapy session should not go ahead today. The AHP discusses the situation with AHA and agrees with this course of action. The above information is listed in the patient notes/electronic file and the subsequent course of action is noted (for example: the AHP may have organised for Mrs. G’s family to pick her up and take her to the doctor for a check up).
8. Cease or modify therapy (cont.) A Grade 3 AHA may adjust therapy activities based on patient performance, where this has been previously discussed with and approved by the AHP. This may include making activities more challenging if the patient is doing well, or simplifying them if the patient is easily achieving goals.
9. Prompt Sometimes patients need more help to achieve success with a task or activity. One way to assist is to use a prompt – a cue or reminder. The prompt gives hints about how to do the activity and can make the difference between whether the patient achieves the goal or not.
9. Prompt (cont.) Prompts can take a variety of forms, including: • Physical assistance – e.g. touching elbow as a guide • Demonstration – performing the task yourself for the patient to then copy • Gestural – e.g. showing a “sh” sign to remind a child to produce this speech sound OR showing a “stop” sign with your hand to show when to end a movement • Positional – e.g. seating the patient so that use of the weaker affected arm is encouraged • Visual – e.g. showing a picture stimulus of how to do the task • Verbal – e.g. describing the steps involved, or reminding the patient what to do
9. Prompt (cont.) It is important to know which type of prompt to use with a patient, as well as how much prompting to use. Too little prompting may mean that the patient cannot achieve success. Too much prompting may make the task too easy and not allow the patient to develop independence with the skill. The AHA should always talk to the AHP about how and when to prompt to ensure therapy sessions are as effective as they can be.
11. Feedback When conducting therapy with patients, it is important to give feedback to the patient about their performance to help the patient achieve their best. Feedback assists patients to know if they are doing the activity in the right way, or if there are any changes they should be making.
11. Feedback (cont.) There are two main types of feedback: • General feedback – e.g. “Well done”, “Good job”, “Good try”, “Keep going, you are doing well” This type of feedback is helpful to provide general encouragement to motivate the patient to keep going. • Specific feedback – e.g. “Lift your leg onto the step”, “Good try. Now let’s see if we can go further next time”, “Whoops, I think you forgot your special “k” sound” This type of feedback gives the patient feedback on exactly what s/he did, which helps them to know what to continue and what to change to achieve success.
11. Feedback (cont.) Discuss with the AHP what type of feedback you should use with the patient to maximise their success in the therapy session.
12 & 13: Responding to patient questions/seeking support The patient may have questions during the therapy session, which may be related to the activities or may be more general about their overall care. Where the question relates to an area within the AHA’s knowledge and experience, the AHA should respond to these questions and provide this information to the patient. The AHA should seek advice from the AHP before responding when the question: • relates to a broader issue • is not within the AHA scope of practice • Is not an area which the AHA has discussed with the AHP
12 & 13: Responding to patient questions/seeking support (cont.) In this situation the AHA could: • ask the AHP to come into the session to talk to the patient • check information with the AHP and report it back to the patient • reschedule the session in consultation with the AHP. If the AHA is not sure, always check with the AHP before giving advice to a patient.