Download
1 / 51
840 likes | 2.18k Views
Otitis Media and Eustachian Tube Dysfunction. R. Kent Dyer, Jr., M.D. Hough Ear Institute Oklahoma City, Oklahoma USA. Incidence of Otitis Media (OM). Most common disease of childhood after viral URI 15 million cases of Acute OM/year in U.S. Cost of treatment: >$5 billion/year.

E N D
Otitis Mediaand Eustachian Tube Dysfunction R. Kent Dyer, Jr., M.D. Hough Ear Institute Oklahoma City, Oklahoma USA
Incidence of Otitis Media (OM) • Most common disease of childhood after viral URI • 15 million cases of Acute OM/year in U.S. • Cost of treatment: >$5 billion/year
Viral or Bacterial Insult Edema Leukocyte Infiltration Purulent Exudate/Granulation Tissue ET Obstruction vs. Resolution Fibrosis Pathology of Acute Otitis Media
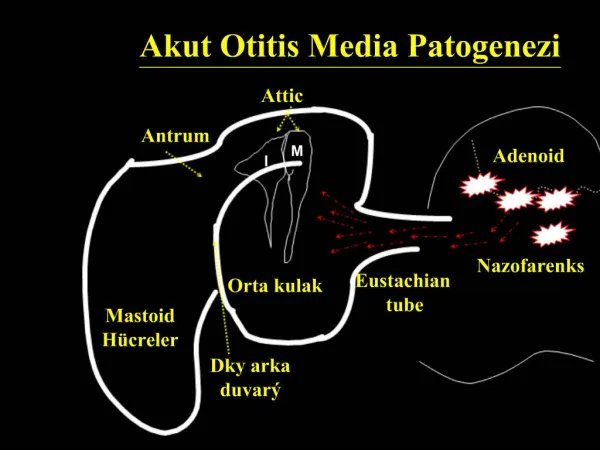
Pathogenesis of Otitis Media • Infection (viral vs. bacterial) • Abnormal eustachian tube function • Allergy (minor role) • Neoplasm (nasopharyngeal carcinoma) • Sinusitis
Eustachian Tube Function • Protection from nasopharyngeal secretions • Ventilation • Clearance of middle ear secretions
Otitis Media Classification • Classified according to: • Duration of disease Acute, subacute, chronic • Quality of effusion Serous, mucoid, purulent • Tympanic membrane appearance
Acute Otitis Media Tympanic membrane: • Opaque • Bulging/injected • Reduced mobility • Purulent effusion
Otitis Media with Effusion Tympanic membrane: • Translucent or opaque • Gray/pink • Reduced mobility • Effusion present +/- air
Chronic Mucoid OM (Glue Ear) Tympanic membrane: • Opaque/gray • Retracted, reduced mobility • Thick effusion, no air • Hearing loss (>20dB HL)
Tympanosclerosis • White plaques in Lamina Propria • Hyaline deposition • Significant conductive hearing loss possible
Atelectasis • Collapse or retraction of tympanic membrane • Often associated with ossicular pathology • Long-standing eustachian tube dysfunction
Attic Retraction • Isolated collapse of Pars Flaccida • May lead to cholesteatoma
Cholesteatoma • Accumulation of squamous epithelium in middle ear & mastoid • Osteolytic enzymes • Often accompanied by chronic otorrhea
Chronic Suppurative Otitis Media • TM Perforation • +/- cholesteatoma • Otorrhea
Pneumatic OtoscopyEssential for Diagnosis of OM Keys: • Air tight seal • Adequate visualization of TM
Tympanometry • Useful for confirming diagnosis (if pneumatic exam inadequate) • Type C (negative peak) Suggests ET dysfunction • Type B (flat) + effusion
Acute Otitis Media Microbiology: • S. pneumoniae 20-30% PCN resistant • H. influenza 30-60% B-Lactamase + • M. catarrhalis 90-95% B-Lactamase +
Chronic Serous Otitis Media Microbiology: • 50% of effusions culture + for bacteria • S. pneumoniae, H. influenza, M. catarrhalis
Chronic Suppurative Otitis Media Microbiology: • P. aeruginosa • S. aureus • Diphtheroids • Klebsiella
Management of Acute Otitis Media • Amoxicillin 90mg/kg/day • Mild PCN allergy (rash) • Cephalosporin • Severe PCN allergy (anaphylaxis) • Azithromycin • Clarithromycin
2nd Line Therapy for Otitis Media • Amoxicillin/Clavulanate • Oral Cephalosporin (2nd or 3rd generation) • Macrolide • Ceftriaxone (IM)
When to Consider 2nd Line Rx • Group day care • Antibiotic Rx within last 30 days • Failure of antibiotic prophylaxis • Refractory AOM Failure to improve with 72 hours
Management of Persistent OM • Watchful waiting 90% of effusions will resolve within 3 months • Additional 2nd line antibiotics • Intranasal steroids • Eustachian tube inflation Valsalva vs. Otovent • Nasal endoscopy
Factors to Considerwith Long-standing Effusions • Degree of hearing loss (>20dB HL) • Vertigo/imbalance • Tympanic membrane changes (retraction) • Speech & language delay • Behavioral changes • Frequency & severity of AOM
Plan of Therapy Amoxil
Plan of Therapy Amoxil If No Improvement in 72 hrs.
Plan of Therapy Amoxil 2nd Line Antibiotic If No Improvement in 72 hrs.
Plan of Therapy Amoxil 2nd Line Antibiotic If No Improvement in 72 hrs. If Persistent Effusion
Plan of Therapy Amoxil 2nd Line Antibiotic 2nd Line Antibiotic/Monitor (up to 3 months) If No Improvement in 72 hrs. If Persistent Effusion
Amoxil 2nd Line Antibiotic 2nd Line Antibiotic/Monitor (up to 3 months) Modify Risk Factors (when possible) & Check Hearing Status If No Improvement in 72 hrs. If Persistent Effusion Plan of Therapy
Amoxil 2nd Line Antibiotic 2nd Line Antibiotic/Monitor (up to 3 months) Modify Risk Factors (when possible) & Check Hearing Status Tympanocentesis usually not indicated If No Improvement in 72 hrs. If Persistent Effusion Plan of Therapy
Indications for Tympanostomy Tubes • >5 episodes of AOM in 6-9 months • Persistent ME effusion x 3 months • Complication of OM • Failure of antibiotic prophylaxis Acute Mastoiditis
Indications for Tympanostomy Tubes • Craniofacial anomaly • Structural changes to TM • Speech & language delay
Choice of Tubes • Short-lasting (6-12 mo.) • Intermediate (12-18 mo.) • Long-lasting (>18 mo.)
Lumen Shaft Medial flange Straight Vent Tube
Flanges Lumen Grommet/Bobbin Style
T TYPE Vent tube Medial Flange Shaft TUBE INDUCED PERFORATION “GOODE T - TUBE” - Xomed
Post-tube Otorrhea • Usually secondary to URI or water exposure • Topical antibiotic usually adequate 5-7 days (Floxin, Ciloxin, Ciprodex)
Water Precautions • Cotton + Vaseline when bathing • Plug • Ear Band-It when swimming
Refractory Otorrhea Consider fungal etiology • Clotrimazole gtts • Amphotericin B powder • Cresylate • Debridement of ear canal • Water Precautions No H2O2!!!
Tube Removal • Removal recommended if tube persists >24 months • Risk of TM perforation 12-25% if tube retained >2 years