Download
1 / 12
190 likes | 785 Views
Hypokalemia. 55 y/o male CC: chronic diarrhea Farmer in La Trinidad, Benguet Noted progressive weakness for the past weeks. Hypokalemia. Urine potassium: 15 meq/L. Diagnostic approach to hypokalemia. Diagnostic approach to hypokalemia. Diagnostic approach to hypokalemia.

E N D
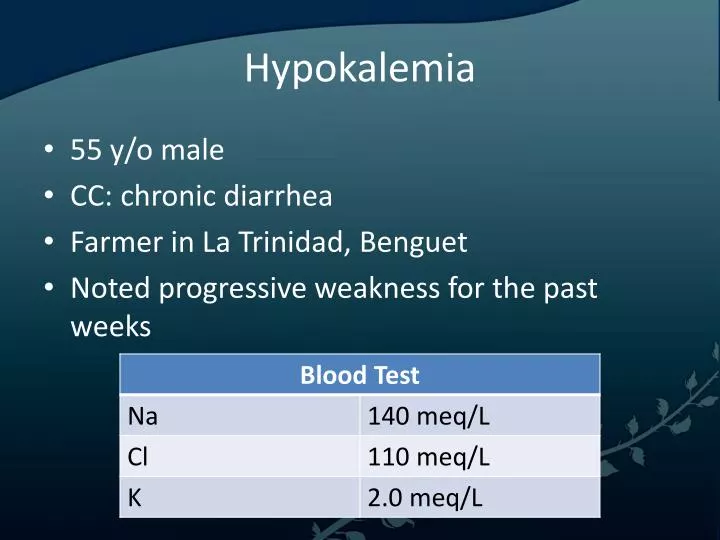
Hypokalemia • 55 y/o male • CC: chronic diarrhea • Farmer in La Trinidad, Benguet • Noted progressive weakness for the past weeks
Hypokalemia • Urine potassium: 15 meq/L
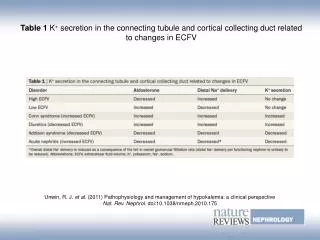
Significance of Urinary K levels • This can be established after eliminating decreased intake and intracellular shift as potential causes of hypokalemia • Appropriate response to K+ depletion is to excrete less than 15 mmol/d of K+ in the urine, due to increased reabsorption and decreased distal excretion • This is exemplified by the diagnostic approach shown previously
Adverse medical implications • More severe hypokalemia may lead to progressive weakness, hypoventilation (due to respiratory involvement involvement, and even complete paralysis • Impaired muscle metabolism and blunted hyperemic response to exercise leads to rhabomyolysis • Leads to prolonged PR interval, decreased voltage and widening of the QRS complex, with increased risk of ventricular arrhythmia
Symptoms of Hypokalemia • Palpitations • Skeletal muscle weakness or cramping • Paralysis, paresthesias • Constipation4 • Nausea or vomiting • Abdominal cramping • Polyuria, nocturia, or polydipsia • Psychosis, delirium, or hallucinations • Depression
Signs of Hypokalemia • Signs of ileus • Hypotension • Ventricular arrhythmias • Cardiac arrest • Bradycardia or tachycardia • Premature atrial or ventricular beats • Hypoventilation, respiratory distress • Respiratory failure • Lethargy or other mental status changes • Decreased muscle strength, fasciculations, or tetany • Decreased tendon reflexes • Cushingoid appearance (eg, edema)
Treatment • ECG monitoring • Establish IV access • Assess respiratory status • Infuse potassium chloride, since his serum potassium is < 2.5 meq/L, in other cases oral is the preferred route for potassium repletion because it is easy to administer, safe, inexpensive, and readily absorbed from the GI tract • Check serum Mg levels since it is difficult to restore K if the former is low