Download
1 / 14
270 likes | 873 Views
HYPOKALEMIA. Andal, Charlotte Ang , Jessy A2. Salient Features. 55 year old, male Diarrhea for several weeks Progressive weakness. Laboratory Findings. Patient. Normal Values. 135-145 meq /L 98-106 meq /L 3.5-5.0meq/L >15 meq /L. Blood Chemistry Na = 140 meq /L

E N D
HYPOKALEMIA Andal, Charlotte Ang, Jessy A2
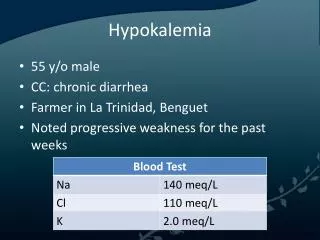
Salient Features • 55 year old, male • Diarrhea for several weeks • Progressive weakness
Laboratory Findings Patient Normal Values 135-145 meq/L 98-106 meq/L 3.5-5.0meq/L >15 meq/L Blood Chemistry • Na = 140 meq/L • Cl= 110 meq/L • K = 2.0 meq/L Urinalysis • K = 15 meq/L
ABG Patient Normal Values 7.45-7.45 35-45 mmHg 22-26 meq/L • pH = 7.28 • pCO2= 39mmHg • HCO3 = 16 meq/L
1. Discuss the diagnostic approach to hypokalemia. What is the cause of hypokalemia in this patient?
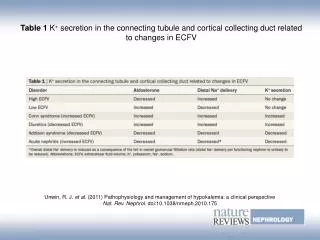
Causes of Hypokalemia • Decreased intake • Starvation • Clay ingestion • Redistribution into cells • Acid-base • Hormonal • Anabolic state • Increased loss • Nonrenal • Renal
Causes of Hypokalemia in the Patient • Increased loss • Nonrenal • Gastrointestinal loss (diarrhea) • Integumentary loss (sweat) • Renal • Increased distal flow • Increased secretion of potassium
Increased renal K excretion • Loss of gastric contents volume depletion and metabolic alkalosis kaliuresis • Hypovolemia stimulates aldosterone release augments K secretion by the principal cells • Filtered load of HCO3 exceeds the reabsorptive capacity of the proximal convoluted tubule increasing distal delivery of NaHCO3 which enhances electrochemical gradient favoring K loss in the urine
2. What are the signs and symptoms of hypokalemia? • Fatigue • Myalgia • Muscular weakness • More severe hypokalemia • Progressive weakness • Hypoventilation • Complete paralysis
3. What are the adverse medical implications of this condition?
5. What is the treatment? • Therapeutic goals: • Correct the K deficit • Minimize ongoing losses
Potassium chloride • Preparation of choice • Promote more rapid correction of hypokalemia and metabolic alkalosis • Potassium bicarbonate and citrate • Tends to alkalinize the patient • More appropriate for hypokalemia associated with chronic diarrhea