Download
1 / 20
200 likes | 563 Views
Evaluation of the Efficacy of Uterine Artery Embolization for Focused Ultrasound Surgery Therapeutic Failures. Alisa Suzuki, MD Brigham and Women’s Hospital, Department of Radiology. Basic Fibroid Treatment Algorithm. asymptomatic. symptomatic. operation. hormone therapy.

E N D
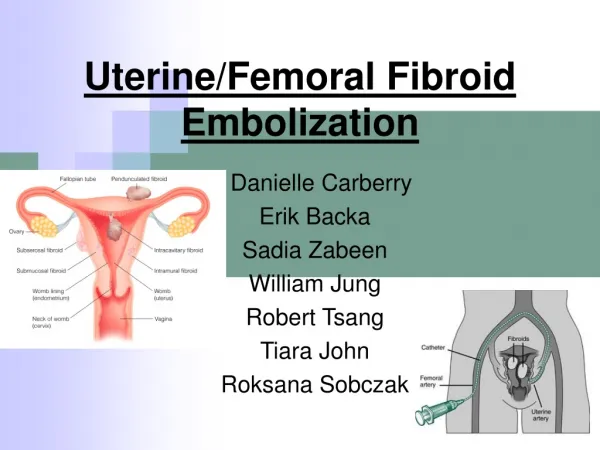
Evaluation of the Efficacy of Uterine Artery Embolization for Focused Ultrasound Surgery Therapeutic Failures Alisa Suzuki, MD Brigham and Women’s Hospital, Department of Radiology
Basic Fibroid TreatmentAlgorithm asymptomatic symptomatic operation hormone therapy Watch carefully MRgFUS laparotomy hysteroscopy laparoscopy UAE hysterectomy TCR stable myomectomy progression T V Hysterectomy observation L Hysterectomy LAVHysterectomy L Myomectomy LA Myomectomy
We evaluate the effect of UAE in patients who are unsatisfied with FUS treatment.
New treatment option from radiology for SYMPTOMATIC FIBROIDS • MR guided Focused Ultrasound Surgery = since 2001 • MRgFUS = a new method ofnon-invasive thermal(heat) ablationfor symptomatic fibroids. • 73% to 91 % of the women who have been treated reported asignificant improvementin their uterine fibroid symptoms. • MRgFUS is an FDA-approved treatmentfor symptomatic uterine fibroids
UAE Procedure POST Procedure
UAE 3 month POST PRE
MRgFUS POST PRE
UAE and MRgFUS - similarities Less or non- invasive compared to conventional gynecological surgeries. = short hospital stay, short recovery = smaller incision, or no incision = No general anesthesia (intravenous conscious sedation) Similar or lower serious adverse event % = High patient satisfaction Performed by a radiologist
? • 73 - 91% of women who have been treated with FUS reported asignificant improvementin their uterine fibroid symptoms. • 9 - 27 % of women did not report clinically satisfactory outcome. 10 patients underwent UAE subsequently at BWH. options : myomectomy, hysterectomy, UAE, re-FUS Patients were allowed to select their treatment.
Study design: • FUS performed in BWH from March 2002 and June 2004. • 7 patients were reviewed. • Pre and post FUS and UAEuterine size. • Pre and post FUS and UAEfibroid size. • Clinicalsymptoms
Result 1 • Size of Fibroid • The mean volume of • pre-FUS fibroid 279cc • 12 month post-FUS fibroid 316cc, -13.0% • post-UAE fibroid 163cc, -49% • Significant decrease in size between post-FUS 12 month size and post-UAE fibroid size. (p=0.02)
Result 2 • Size of Uterus • The mean volume of • pre-FUS uterus 617 cc • Post-FUS 12 month uterus 682 cc, +10.0% • post-UAE uterus was 475cc, - 31% • Significant decrease in uterine size betweenpre-FUS and post UAE. (p=0.03) • Significant decrease in size between 12 month post-FUS fibroid size and post-UAE fibroid size. (p=0.002)
Result 3 Clinical symptoms Clinical symptoms including heavy bleeding, bulk, and pelvic pressure wereimproved in all patients. (as reported by patient)
@ FUS Nov-2003 Post FUS Gd Image These two fibroids were targeted.
Post FUS 6 & 13 months May- 04, 6 month follow up. Uterus size 12.1 x 11.7 x 9.8 cm, 721cc Jan -05, 13 month follow up. Uterus size 14.4 x 12.4 x 7.8 cm, 738cc
@ UAE, Post FUS 23 months Dec-05 UAE.
Post UAE 13 months, Post FUS 36 month Jan -05, Post FUS13 monthfollow up. Uterus size 14.4 x 12.4 x 7.8 cm, 738cc Nov-06 Post FUS36 m, post UAE 13 m follow up. Uterine size 11.4 x 9.6 x 8.4 cm, 487.2cc
UAE can be therapeutic after unsatisfactory outcomes of FUS. MRg FUS is a new, exciting technique which can ‘zap’ fibroids in 3 hours while the patient is sleeping on the MRI table. Patients who develop clinical failure after FUS treatment could subsequently receive full benefit from Uterine Artery Embolization. Now we can comfortably inform patients that an FUS treatment failure does not require subsequent highly invasive surgery procedure as a minimally invasive procedure (like UAE) may resolve the patient's symptoms.
There are many areas where our experience with FUS is limited. • Due to the newness of FUS, there is limited long-term follow up data on patients.