Download
1 / 17
190 likes | 397 Views
Statin Landmark Trials Across the Spectrum of Risk: Secondary CV Prevention . TNT: Study Design Treating to New Targets. Patient Population. Clinically evident CHD LDL-C 130 250 mg/dL following up to 8-week washout and 8-week open-label run-in with atorvastatin 10 mg.

E N D
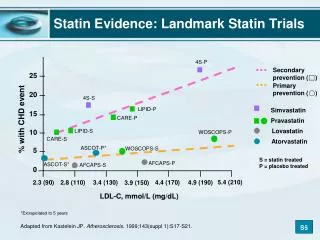
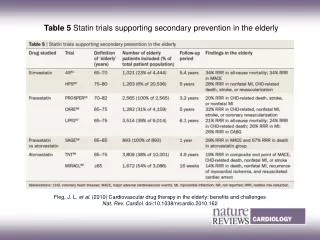
Statin Landmark Trials Across the Spectrum of Risk: Secondary CV Prevention
TNT: Study Design Treating to New Targets Patient Population • Clinically evident CHD • LDL-C 130250 mg/dL following up to 8-week washout and 8-week open-label run-in with atorvastatin 10 mg Atorvastatin 10 mg LDL-C target: 100 mg/dL 10,001 Patients Primary End Point Atorvastatin 80 mg LDL-C target: 75 mg/dL • Time to first occurrence of a major cardiovascular event (CHD death, nonfatal non–procedure-related MI, resuscitated cardiac arrest, fatal or nonfatal stroke) 5 years LaRosa JC et al. N Engl J Med. 2005;352:1425-1435.
TNT Primary Efficacy Outcome Measure:Major Cardiovascular Events* 0.14 HR = 0.78 (95% CI, 0.69–0.89) P < .001 0.12 Atorvastatin 10 mg (n = 5006) LDL-C 101 mg/dL (2.6 mmol/L) 0.10 0.08 Cumulative Incidence of Major Cardiovascular Events, % 0.06 Atorvastatin 80 mg (n = 4995) LDL-C 77 mg/dL (2.0 mmol/L) 0.04 0.02 Relative risk reduction = 22% 0 0 1 2 3 4 5 6 Time, years *CHD death, nonfatal non–procedure-related MI, resuscitated cardiac arrest, fatal or nonfatal stroke. LaRosa JC et al. N Engl J Med. 2005;352:1425-1435.
TNT: Primary and Secondary Efficacy Outcomes Primary Efficacy Measure HR P Value Major CV event 0.78 .001 CHD death 0.80 .09 Nonfatal non–procedure-related MI 0.78 .004 Resuscitated cardiac arrest 0.96 .89 Fatal/nonfatal stroke 0.75 .02 Secondary Efficacy Measures Any cardiovascular event 0.81 <.001 Major coronary event* 0.80 .002 Any coronary event 0.79 <.001 Cerebrovascular event 0.77 .007 Hospitalization for CHF 0.74 .01 Peripheral arterial disease 0.97 .76 All-cause mortality 1.01 .92 Atorvastatin 80 mg Better Atorvastatin 10 mg Better *CHD death, nonfatal non–procedure-related MI, resuscitated cardiac arrest. LaRosa JC et al. N Engl J Med. 2005;352:1425-1435.
Atorvastatin 10 mg Atorvastatin 80 mg TNT: Time to First Fatal or Nonfatal Stroke 0.04 HR = 0.75 (95% CI 0.59-0.96) P=0.02 0.03 Relative RR = 25% Proportion of patients experiencing events 0.02 0.01 0 0 1 2 3 4 5 6 Time (years) LaRosa JC et al. N Engl J Med. 2005;352:1425-1435.
TNT: Safety Profile 10 P<0.001 8.1 8 P =0.72 5.8 6 4.8 4.7 % of Patients 4 P<0.001 1.2 2 0.2 (n=9) (n=406) (n=289) (n=241) (n=234) (n=60) 0 Treatment-Related Adverse Events Treatment-Related Myalgia Elevated Liver Enzymes* Atorvastatin 80 mg (n=4,995) Atorvastatin 10 mg (n=5,006) Persistent = 2 consecutive measurements. LaRosaJC et al. N Engl J Med. 2005;352:1425-1435.
IDEAL (Incremental Decrease in EndPoints Through Aggressive Lipid Lowering): Study Design Patient Population • Previous hospitalization with definite acute MI or a history of definite MI • Eligibility for statin therapy according to respective national guidelines at discharge Atorvastatin 80 mg 8888 Patients Primary End Point Simvastatin 20 mg; titrationto 40 mg for TC >190 mg/dL • Time to occurrence of a major cardiovascular event (CHD death, nonfatal acute MI, resuscitated cardiac arrest) 4.8 years Open label with blinded end-point evaluation Pedersen TR et al. JAMA. 2005;294:2437-2445.
IDEAL: Primary and Secondary End Points Major coronary events – primary end point Major CV events – secondary end point 16 16 Simvastatin Atorvastatin Simvastatin Atorvastatin 13%RRR 12 12 11%RRR Cumulative Hazard, % Cumulative Hazard, % 8 8 4 4 HR = 0.89 (95% CI, 0.76–1.01) P = .07 HR = 0.87 (95% CI, 0.78–0.98) P = .02 0 0 0 1 2 3 4 5 0 1 2 3 4 5 Years Since Randomization Years Since Randomization Any coronary event – secondary end point Any CV event – secondary end point 40 40 Simvastatin Atorvastatin Simvastatin Atorvastatin 16%RRR 30 30 16%RRR Cumulative Hazard, % Cumulative Hazard, % 20 20 10 10 HR = 0.84 (95% CI, 0.78–0.91) P < .001 HR = 0.84 (95% CI, 0.76–0.91) P < .001 0 0 0 1 2 3 4 5 0 1 2 3 4 5 Years Since Randomization Years Since Randomization The primary end point of IDEAL (a composite of CHD death, nonfatal MI, and resuscitated cardiac arrest) did not reach statistical significance (HR = 0.89; 95% CI, 0.78-1.01; P = 0.07). Pedersen TR et al. JAMA. 2005;294:2437-2445.
Effects of Atorvastatin 80 mg/d vsSimvastatin 20 to 40 mg/d on Any CV Event SubjectsWithEvent Relative RiskReduction (%) PValue Events HR (95% CI)* 2546104841619293 (0.77 – 0.90) <.0001 1st 17 (0.67 – 0.86) 2nd 24 <.0001 (0.67 – 0.99) 3rd 19 .035 (0.57 – 1.01) 4th 24 .058 (0.48 – 1.09) 5th 28 .117 0.50 0.75 1.25 1.50 1.0 Atorvastatinbetter Simvastatinbetter *Adjusted for sex and age at baseline. Tikkanen MJ et al. J Am Coll Cardiol. 2009;54:2353-2357.
MIRACL (Myocardial Ischemia Reduction With Aggressive Cholesterol Lowering): Study Design Patient Population • Non-Q-wave MI orunstable angina • Randomized 24–96 hoursfrom admission Atorvastatin 80 mg 3086 Patients Primary End Point Placebo • Time to ischemic events (CHD death, nonfatal MI, documented angina requiring hospitalization) 16 weeks double-blind Schwartz GG et al. JAMA. 2001;285:1711-1718.
MIRACL: Primary Efficacy Measure—Time to First Event* 17.4% 16% RRR Placebo (n = 1548) LDL-C 135 mg/dL (3.5 mmol/L) 15 14.8% Atorvastatin 80 mg (n = 1538) LDL-C 72 mg/dL (1.9 mmol/L) 10 Cumulative Incidence, % 5 RR = 0.84P = .048 95% CI, 0.701–0.999 0 0 4 8 12 16 Time Since Randomization, weeks *Death (any cause), nonfatal MI, resuscitated cardiac arrest, worsening angina with new objective evidence and urgent rehospitalization. Schwartz GG et al. JAMA. 2001;285:1711-1718.
MIRACL: Stroke Water DD et al. Circulation. 2002;106:1690-1695.
PROVE IT-TIMI (Pravastatin or Atorvastatin Evaluation and Infection Therapy–Thrombolysis in Myocardial Infarction) 22: Study Design Patient Population • Hospitalized for an acute coronary syndrome in the preceding 10 days • TC ≤240 mg/dL (6.2 mmol/L) or TC ≤200 mg/dL (5.2 mmol/L) if receiving lipid-lowering therapy Atorvastatin 80 mg 4162 Patients Primary End Point Pravastatin 40 mg • Time to first occurrence of a major cardiovascular event (death from any cause, MI, unstable angina, revascularization, stroke Double-blind 925 primary end points Cannon CP et al. N Engl J Med. 2004;350:1495-1504.
PROVE IT: Primary End Point (All-Cause Death or Major CV Events in All Randomized Subjects) 26.3% 30 16% RRR (P = .005) Pravastatin 40 mg (n = 1548) 95 mg/dL (2.5 mmol/L) 25 22.4% 20 Atorvastatin 80 mg (n = 2099) 62 mg/dL (1.6 mmol/L) 15 –35% LDL reduction Death or Major CV Event, % 10 5 0 30 0 12 15 18 21 24 27 3 6 9 Months of Follow-up Major CV event = MI, unstable angina requiring rehospitalization, revascularization, or stroke. Cannon CP et al. N Engl J Med. 2004;350:1495-1504.
12 10 8 6 4 2 0 0 PROVE IT-TIMI 22: Intensive Therapy With Statins in Patients With ACS: Early and Long-term Benefits Month 6 to end of study Randomization to 30 days 5 n = 1752 RRR = 28% P = .003 4 n = 2063 RRR = 28%P = .046 3 Composite triple end point* (%) n= 1812 Composite triple end point* (%) n = 2099 2 1 0 5 10 15 20 25 30 6 12 18 24 Days following randomization Months following randomization Pravastatin 40 mg Atorvastatin 80 mg *Death, MI, or rehospitalization with recurrent ACS. Adapted from Ray KK et al. J Am Coll Cardiol. 2005;46:1405-1410.
Safety of Atorvastatin 80 mg in Clinical Trials *Consecutive measurements. †Newman C et al. Am J Cardiol.2006;97:61-67; Cannon CP et al. N Engl J Med. 2004;350:1495-1504; LaRosa JC, et al. N Engl J Med. 2005;352:1425-1435; Pedersen TR et al; for the IDEAL Study Group. JAMA. 2005;294:2437-2445; Amarenco P et al. N Engl J Med. 2006;355:549-559.
Overview of Adverse Events forAtorvastatin 10 mg and 80 mg and Placebo Newman C et al. Am J Cardiol. 2006;97:61-67.