Download
1 / 33
330 likes | 470 Views
Asians and Pacific Islanders and HIV. Jason Tokumoto, MD Assistant Clinical Professor of Medicine University of California at San Francisco. Case Presentation . KC is a 32 year-old Chinese American gay male with AIDS.

E N D
Asians and Pacific Islanders and HIV Jason Tokumoto, MD Assistant Clinical Professor of Medicine University of California at San Francisco
Case Presentation • KC is a 32 year-old Chinese American gay male with AIDS. • He initially presented to a dermatologist because of purplish skin lesions which on biopsy proved to be Kaposi’s sarcoma. He had these lesions for 6 months before seeking care. His CD4 cell count was 30 and viral load 200,000.
Case Presentation • KC became progressively ill despite anti-retroviral therapy developing CMV retinitis, disseminated MAC, worsening Kaposi’s sarcoma despite appropriate treatment. • In need of increasing care and help but did not want to access the services of HIV community based organizations. • Family in New York. Not aware of his HIV status. He informed his family he had a “bad cancer.”
Case Presentation • KC decided that he wanted to return to New York. His family also wanted him to return home so that they could take care of him. • He and I had several long discussions about telling his family about his HIV status since they were going to be taking care of him and that they should be informed. • He agreed but wanted me to tell his family.
Case Presentation • His mother came to San Francisco to take KC home. • She did not speak or understand English so an interpreter was used. • When she saw her son for the first time, she was shocked to see the condition he was in. She thought it was due to the “bad cancer.”
Case Presentation • It took 6 months for KC to seek medical care. • He was not able to disclose his HIV status to his family. • He did not want to access services provided by community organizations. • He could not tell his mother directly that he had AIDS.
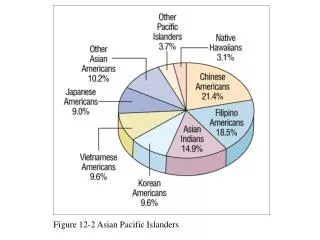
Epidemiology-USA, December 1998 • 4,974 APIs with AIDS • 89% men • 79% of these men were gay • 59% foreign born
Epidemiology—USA, December 1998 • Five states, which account for 63% of the API population in the USA, reported 78% of the cases: • California 45% • Hawaii 12% • New York 15% • Texas 3% • Washington 3%
Epidemiology—USA, December 1998 • Incidence rate per 100,000 for 1996-1997: • Highest rate in Northeast 15.9 • West 13.8 • South 10.6 • Midwest 5.7
Epidemiology-USA • There are still 40,000 new infections per year. • 20-30% of those infected are unaware that they are infected. • Illegal immigrant from Asia not seeking testing because of concern about being deported.
Testing of APIs • Rate of PCP in New York City between 1997-1998: • Caucasians decreased by 50% • African Americans decreased by 40% • Latinos decreased by 40% • APIs increased by 30% • Because PCP is preventable, why this high rate?
Testing of APIs • Nonseeking of or delay in seeking health care may partly explain this high rate. • Cultural stigma • Family abandonment/shame • Perceptions of social norm regarding homosexuality • Belief in Karma(a sense of fatalism) • Low levels of acculturation • Possible deportation because of one’s illegal alien status
Testing of APIs—APIWC, San Francisco • 1999-APIs accounted for only 9% undergoing HIV testing at various public health department sites in San Francisco • APIWC HIV Testing and Training Program started offering free HIV testing(OraSure) at various events( eg API events—Vietnamese TET Festival, gay parade, massage parlors). The target population is primarily APIs but no one is turned away for testing.
Testing of APIs--APIWC, San Francisco • Advertising of HIV testing • During the 1st year (2000-2001), 366 tests done(majority were APIs and having their first HIV test) • Of the 366, 8 were HIV positive
Cultural diversity • In the USA, APIs consists of 49 ethnic groups speaking over 100 languages and dialects. • Although there are some basic similarities among these groups, each group is distinct and each has it’s unique specific “values.” • Keeping these cultural factors in mind and being sensitive about these factors can help to facilitate your care of APIs.
Cultural issues • Family role • Often overides individual identity. • Ones behavior reflect upon one’s ancestors as well as the entire family, community and ethnic group. • Family members are responsible and obligated to the family. • Filial piety—obligation an individual has towards ones parents.
Cultural issues • Family role/Filial piety • Hide or ignore HIV diagnosis • Fail to seek or adhere to treatment • Not seek social services • Isolate from family
Cultural issues • Shame • Often used to remind individuals of their obligation to their families. • For many Asians, shame is often understood as “losing face.”
Cultural issues • Shame • Patient often feels shame about having HIV and have disappointed their families and therefore will hide their HIV diagnosis. • Feel unworthy of receiving care. • To “save face” a patient will try to appear that everything is okay and that he/she has no needs.
KC—Family role and shame • Not able to disclose is HIV status and homosexuality because of fear of bringing shame to his family. • KC suspected that he was HIV-infected but delayed getting medical care because of fear of bringing shame to his family.
Cultural issues • Avoid expressing one’s feelings • Discourages direct communication of feelings. • Talking about one’s feelings often viewed as a sign of weakness.
Cultural issues • Avoid expressing one’s feelings • Can compound a patient’s sense of isolation and alienation
KC—avoid expressing one’s feelings • KC was quite stoic when his mother was informed of his HIV status. • Seeking help was a sign of weakness.
Cultural issues • Indirect communication • Express one’s desires through silence or non-verbal communication and therefore the provider who expects the patient to speak up and say what is on his/her mind may miss what is being communicated.
Cultural issues • Language • Can isolate a patient from seeking medical care • Use of an intepreter—patient may be reluctant to discuss sensitive issues • Professional medical interpreters may have their own cultural biases regarding HIV
Cultural issues • Deference to Authority • May see physician as “God” • May only appear to be compliant in order to please their provider • Can be barrier to self-advocation
Cultural issues • Taboo Subjects • Sex, sexuality, homosexuality considered taboo in many API cultures • Emphasis on handling problems associated with these subjects privately • Avoiding these topics with a provider can result in medical and social service needs not being met
Cultural issues • Herbs and Drug Therapy • Southeast Asian Americans often believe medications should be given on a short term basis with expectation of immediate relief • Asian Americans more likely to develop side effects from psychotropic drugs and to fear that antidepressant medication will make them too drowsy • Traditional healing modalities such as acupuncture, qi gong may increase their sense of well-being
Interventions • “Culturally sensitive care” • To develop trust, medical provider should proceed slowly • Validate and even encourage using both Western and traditional treatment • Review possible outcomes of both Western and traditional treatment
Interventions • “Culturally sensitive” care • A patient’s culture should be seen as a potential asset rather than as a barrier • Link patients to culturally sensitive services • Educate providers about culturally sensitive services
Interventions • Peer intervention • Meeting other APIs living with HIV will give a sense of not being alone and help to find others who share a common cultural background • Educate patient • Explaining the medical system and provider/patient role can help the patient to learn to advocate for his or her self. Teach patients to question authority and analyze what they read or hear
The Golden Rule • Buddhism • “Hurt not others in ways that you yourself would find hurtful.” • Confucianism • “Do not unto others what you would not have them do unto you.” • Islam • “No one of you is a believer until he desires for his brother that which he desires for himself.” • Judism • “What is hateful to you, do not to your fellowman.” • Christianity • “Do unto others as you would have them do unto you.”