Download
1 / 39
471 likes | 1.21k Views
PREVENTION STRATEGY FOR POSTDURAL PUNCTURE HEADACHE (PDPH). Berrin Gunaydin, MD, PhD Department of Anesthesiology and Reanimation Faculty of Medicine-Gazi University Ankara-Turkey. AIM.

E N D
PREVENTION STRATEGY FOR POSTDURAL PUNCTURE HEADACHE(PDPH) Berrin Gunaydin, MD, PhD Department of Anesthesiology and Reanimation Faculty of Medicine-Gazi University Ankara-Turkey
AIM • Anesthetic management of a parturient after unintentional dural puncture during epidural insertion for cesarean delivery and strategy to prevent PDPH Gunaydin & Karaca. Acta Anaesthesiol Belg 2006;70:823-30
Case Report Parturient • ASA II, 26 year-old primigravid • 38 weeks of gestation • 69 kg and 167 cm Preparation for Epidural Anesthesia • 10 ml/kg Ringer lactate infusion • 10 mg metoclopramide and 50 mg ranitidin iv • Monitorization (heart rate, blood pressure, peripheral oxygen saturation) Gunaydin & Karaca. Acta Anaesthesiol Belg 2006;70:823-30
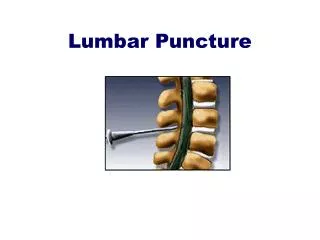
Case Report Epidural Anesthesia • Epidural 18 G Touhy needle, 20 G catheter • Loss of resistance to saline • Between L2-3 intervertebral space • Sitting position by midline approach • Accidental dural puncture at 4.5 cm depth • Suddenly spontaneous backflow of CSF in the loss of syringe Gunaydin & Karaca. Acta Anaesthesiol Belg 2006;70:823-30
Management • Initially,CSF in the syringe was injected back into the subarachnoid space • 7.5 mg of hyperbaric bupivacaine with 20 µg of fentanyl was injected into the subarachnoid space through epidural needle • Then, epidural needle was removed Gunaydin & Karaca. Acta Anaesthesiol Belg 2006;70:823-30
Resiting epidural catheter • Between L3-4 intervertebral space for further top-up and/or postoperative analgesia • Sensory block level was T10 • Therefore, following epidural test dose administration (3 ml 2% lidocaine including 5 µg/ml adrenaline) 3 ml 0.5% plain bupivacaine was given through the epidural catheter • Then, sensory block reached to T4 and surgery was allowed Gunaydin & Karaca. Acta Anaesthesiol Belg 2006;70:823-30
Further Management • Epidural catheter was kept in situ for 48 hours • When sensory blocked regressed to T10, PCA pump was connected PCA settings • 4 ml/h basal infusion of 0.125% bupivacaine with 2 µg/ml fentanyl • 10 min lock-out • 6 ml bolus on demand • 35 ml for 4 h limit Gunaydin & Karaca. Acta Anaesthesiol Belg 2006;70:823-30
Further Management • Epidural catheter was removed after 48 hours • Parturient received 370 ml PCA solution • No PDPH was observed Gunaydin & Karaca. Acta Anaesthesiol Belg 2006;70:823-30
Pathophysiology of PDPH • Total volume of CSF in an adult 150 mL • 50% of which is in the cranium • 75 ml supraspinal, 75 ml spinal • 450-500 mL of CSF is produced daily(0.35 ml/min) • CSF pressure in the lumbar region • in the supine position is between 5 to 15 cmH2O • in the vertical position it exceeds 40 cmH2O
Mechanism of PDPH There are no pain receptors in the brain itself Headaches are often caused by irritation of dura CSF cushions the brain by filling the subarachnoid space
Mechanism of PDPH • Persistent CSF loss through the hole • Decrease in the CSF volume and/or pressure leading to shift of the intracranial contents and traction on the pain sensitive structures • Loss of cushion effect
Mechanism of PDPH ContinuousCSF loss/leakage Subarachnoid pressure may be reducedto 4 cmH2O Activation of adenosine receptors (arterial and venous vasodilatation) rate of CSF lossrate of CSF production (0.084-4.5 ml/sec) > (0.35 ml/min=0.0058 ml/sec) PDPH
Symptoms of PDPH Severe cephalgia PDPH Photophobia Nausea-vomiting Dizziness Neck stiffness Tinnitus Diplopia Hearing loss
WHAT HAPPENS? CSF Loss/leakage Intracranial hypotension Intracranial haemorrhage
Patient history & symptoms Usually frontal in origin, radiates to occiput Exacerbated by sitting or standing (postural) Dramatically relieves in the supine position (standard diagnostic criterion) Diagnostic lumbar puncture Low CSF opening pressure “dry tap” Slightly raised CSF protein Rise in CSF lymphocyte MRI extradural collection of CSF CT myelography Retrograte radionuclide myelography Csyternography Diagnosis
Non-specific headache Migraine Caffeine withdrawal headache Meningitis chemical or infective Sinus headache Drugs amphetamine, cocaine Pneumocephalus Preeclampsia Pituitary apoplexy Cerebral vein thrombosis Subdural hematoma Intracranial tumour Differential Diagnosis
Prevention Strategies Prevention strategies differ depending on the timing of dural puncture • After intentional spinal • After unintentional epidural needle insertion into subarachnoid space
Preventive ConceptsAfter intentional dural puncture Use • atraumatic spinal needles without age limits • proper needle material • finer gauge in predisposed patients
Prevention StrategiesFor inadvertent dural puncture during epidural Baraz & Collis. Management of accidental dural puncture.A survey of UK practice. Anaesthesia 2005 • Insertion of the epidural catheter into the subarachnoid space through the hole • Resiting the epidural catheter • Bed rest & supportive therapy • Drug therapy • Prophylactic • epidural saline • İntrathecal saline • epidural blood patch (EBP)
Intrathecal catheters • Leaving the catheter promote an inflammatory response to seal the hole • Norris & Leighton Failed to show it because they removed the catheter immediately after vaginal delivery • Liu • left the catheter in place for 12-24h • demonstrated low risk of developing PDPH
Sequential Strategy for intrathecal catheter use • Injection of CSF back into subarachnoid space through the epidural needle • Insertion of an epidural catheter into subarachnoid space • injection of saline of 3-5 mL into subarachnoid space through the subarachnoid catheter • Administration of bolus, then continuous intrathecal analgesia • Leaving the catheter in situ in the subarachnoid space for a total of 12-20 h Kuczkowski & Bneumof.Acta Anaesthesiol Scand 2003; 47:98-100 (n=7, 14%) Kuczkowski. Minerva Anestesiol 2004;70:823-30 (n=15, 6.6%)
11 trials, among 1723 patients • Immediate mobilization vs bed rest • 31% bed rest vs (27%) early mobilization
Posture & fluids for preventing PDPH Comfortable position should be encouraged Supine????? Prone is advocated Sudlow &Warlow Cochrane Database Syst Rev 2002
Drug therapy • Caffeine (oral/iv) • Theophylline (oral) • Sumatriptin (SC) • Vasopressine (IM) • Synthetic analog, DDAVP=Desmopressine acetate, IM • ACTH Thurnbull & Shephard. Br J Anaesth 2003;91:718-29
Drug therapyCaffeine • Crosses blood brain barier • Central nerve system stimulant • Cerebral vasoconstrictor • 300-500 mg oral/iv once/twice daily • t1/2=3-7.5 h, LD50=150 mg/kg • at 4h,decrease in the severity of symptoms • at 24h, no difference in severityof symptoms • no difference in the need for EBP 50-100 mg caffeine 0.150g/L caffeine 330 mL 49.5 mg caffeine/330 ml
Theophylline Member of methylxantine family Long acting oral preparations Potent cerebral vasoconstrictor Increase CSF production by stimulating the Na-K pumps Sumatriptin 5HT1D receptor agonist Cerebral vasoconstrictor Advocated for migraine Expensive SC injection (6 mg) t1/2= 2 h Drug therapy Kuczkowski. Arch Gynecol Obstet 2006
Drug therapyDrugs targeting mast-cell inactivation ACTH • Presumably downregulation of CRH (potent mast-cell activator) • 1.5 µg/kg infusion Hydroxycine • Antihistaminic drug established for premedication • Mast-cell stabilising and anxiolytic properties Tricyclic antidepressants (amitriptylin, doxepin) • Analgesic (partially by mast-cell inhibitory effect) Selective CB-2-R agonists • Not yet available, but promising
Prophylactic epidural/intrathecal saline Prophylactic epidural saline/RL • 1-1.5 liter/24 h is started on the 1st day after dural puncture • It is infused up to 35 ml/h for 24-28 h Prophylactic intrathecal saline • Immediate injection of 10 ml intrathecal saline after wet tap significantly reduced PDPH Charsley et al. Reg Anesth Pain Med 2001;26:301-305
Sudlow &Warlow Cochrane Database Syst Rev 2002EBP for preventing & treating PDPH • Epidural blood patch (n=32) vs sham patch (n=32) • No decrease in the incidence of PDPH • No need for therapeutic EBP was detected • Prophylactic EBP did shorten PDPH symptoms
Treatment Goals for PDPH • Replace the lost CSF fluid • Seal the puncture site • Control the vasodilation with cerebral vasoconstrictor drugs
Clinical presentation of PDPHSeverity of PDPH should be evaluated • Mild PDPH (VNS score 1-3) • slight restriction of daily activities • the patient is not bedridden, no associated symptoms • Moderate PDPH (VNS score 4-7) • significant restriction of daily activities • the patient is bedridden part of the day • associated symptoms may or may not be present • Severe PDPH (VNS score 8-10) • incapacitating headache • impossible to sit up • associated symptoms are always present
Epidural saline Infusion/bolus Inert/sterile Mass effect 30 ml bolus saline once 10-120 ml bolus saline via caudal epidural Saline may induce an inflammatory reaction Epidural Dextran 40 infusion or bolus High molecular weight Viscosity Sustained tamponade around dural perforation No inflammatory response that would promote healing TreatmentAfter established PDPH
Epidural Blood Patch (EBP) • History (Gormley 1960, DiGiovanni & Dunbar 1970) • Mechanism of action Plug theory Clot is formed by injecting 15-20 ml autologous blood in the epidural space to provide adherence to the dura mater and directly patches the hole Pressure patch hypothesis Volume of blood injected into epidural space increases CSF pressure leading to reduction in the traction of the pain sensitive brain structures
Contraindications of EBP Infection on the back Sepsis Coagulopathy Raised white cell count Prexia Patient refusal Indication Failed conservative treatment Timing Beyond 24 h after dural puncture Recumbent positioning For 2 h after patching may improve the efficacy EBP
EBP • Complication rate is rare • ~35% transient backache • Success rate is ~94% (70-98%) • 90% initial relief • 61-75% persistent relief • Repeat EBP has a similar success rate • Reverse the complications of dural puncture
Treatment • It is recommended not to delay EBP more than 24 h after the diagnosis of severe PDPH
Fibrin glue • May be placed blindly or CT guided percutanous injection Crul et al. Anesthesiology 1999; 91: 576-7
Conclusions Gunaydin & Karaca. Acta Anaesthesiol Belg 2006;70:823-30 • PDPH is of interest in the obstetric population undergoing cesarean delivery • In the event of recognized wet tap during epidural insertion, prevention of PDPH should be considered • Initial intrathecal saline injection might prevent immediate CSF loss and intrathecal drug injection allows onset of anesthesia • Resiting the epidural catheter and then keeping it postoperatively connected to PCA pump might decrease the incidence of PDPH