Download
1 / 36
751 likes | 2.87k Views
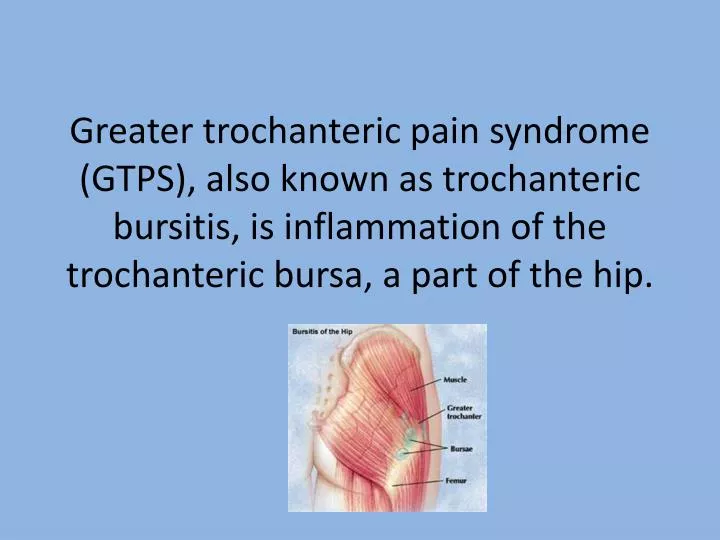
Greater trochanteric pain syndrome (GTPS), also known as trochanteric bursitis, is inflammation of the trochanteric bursa, a part of the hip. Anatomy.

E N D
Greater trochanteric pain syndrome (GTPS), also known as trochanteric bursitis, is inflammation of the trochanteric bursa, a part of the hip.
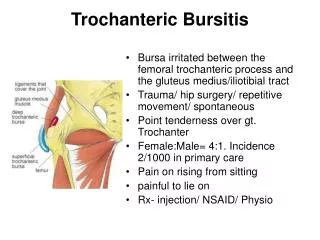
Anatomy • This bursa is situated adjacent to the femur, between the insertion of the gluteus medius and gluteus minimus muscles into the greater trochanter of the femur and the femoral shaft. • It has the function, in common with other bursae, of working as a shock absorber and as a lubricant for the movement of the muscles adjacent to it.
Causes • often the lateral hip pain is caused by disease of the gluteal tendons which secondarily inflames the bursa. • This is most common in middle-aged women and is associated with a chronic and debilitating pain which does not respond to conservative treatment. • Other causes of trochanteric bursitis include uneven leg length, iliotibial band syndrome, and weakness of the hip abductor muscles.
GTPS • can remain incorrectly diagnosed for years, because it shares the same pattern of pain with many other musculoskeletal conditions. • Thus people with this condition may be labeled malingerers, or may undergo many ineffective treatments due to misdiagnosis. It may also coexist with low back pain, arthritis, and obesity.
Prevention • Because wear on the hip joint traces to the structures that support it (the posture of the legs, and ultimately, the feet), proper fitting shoes with adequate support are important to preventing GTPS. • For someone who has flat feet, wearing proper orthotic inserts and replacing them as often as recommended are also important preventive measures. • Strength in the core and legs are also important to posture, so physical training also helps to prevent GTPS. But it is equally important to avoid exercises that damage the hip.
Diagnosis • A doctor may begin the diagnosis by asking the patient to stand on one leg and then the other, while observing the effect on the position of the hips. • Palpating the hip and leg may reveal the location of the pain, and range-of-motion tests can help to identify its source.
Background • Trochanteric bursitis is characterized by painful inflammation of the bursa that is located just superficial to the greater trochanter of the femur. • Patients typically complain of lateral hip pain, although the hip joint itself is not involved, because pain may radiate down the lateral aspect of the thigh.
Pathophysiology • Inflammation of the affected bursa between the femoral trochanteric process and the gluteus medius/iliotibial tract may be due to acute or repetitive (cumulative) trauma. • .
Pathophysiology • Acute trauma includes contusions from falls, contact sports, and other sources of impact.
Pathophysiology • Repetitive trauma includes bursal irritation due to friction by the iliotibial band (ITB), which is an extension of the tensor fascia lata (TFL) muscle. • Such repetitive, cumulative irritation often occurs in runners, but it can also be seen in less-active individuals
Pathophysiology • Other predisposing factors include leg-length discrepancy, hip abductor weakness, and lateral hip surgery.
Greater Trochanteric Pain Syndrome(GTPS) • (GTPS) is now being commonly substituted for trochanteric bursitis, because the inflammatory etiology of the pain is being refuted by current research using ultrasound, magnetic resonance imaging (MRI), and histologic evidence.
Frequency • Trochanteric bursitis (greater trochanteric pain syndrome, GTPS) is relatively common among physically active and sedentary patients and can occur as a complication of arthroscopic surgery of the hip. The overall complication rate has been estimated to be 1.4%. • The prevalence of unilateral trochanteric bursitis (greater trochanteric pain syndrome, GTPS) is 15.0% in women and 8.5% in men and that of bilateral GTPS is 6.6% in women and 1.9% in men.
Demographics • Race No racial predilection has been reported. • Sex A study published in a British journal reported that there appeared to be a female preponderance (80%) of trochanteric bursitis (greater trochanteric pain syndrome, GTPS) relative to males. • Age Trochanteric bursitis (greater trochanteric pain syndrome, GTPS) can occur in adults of any age. • Lievenseet al reported the annual incidence of trochanteric pain in primary care settings was 1.8 patients per 1000.
Sport-Specific Biomechanics • Athletic activities that are potentially associated with trochanteric bursitis (greater trochanteric pain syndrome, GTPS) include those involving running or sports that are associated with the possibility of falls and/or physical contact.
Sport-Specific Biomechanics • Other contributing factors may include running on banked surfaces, which essentially produces a functional leg-length discrepancy because the contact surface of the downhill foot is lower.
History • In cases of acute trauma, patients may recall the specific details of the impact that caused the injury. • The classic symptom of trochanteric bursitis (greater trochanteric pain syndrome, GTPS) is pain at the greater trochanteric region at the lateral hip. • The pain may radiate down the lateral aspect of the ipsilateral thigh but usually does not radiate all the way into the foot. • Typically, symptoms worsen when the patient is lying on the affected bursa (eg, lying in the lateral decubitus position on the affected side). • Pain may awaken the patient at night.
Physical • The most classic finding in trochanteric bursitis (greater trochanteric pain syndrome, GTPS) is the elicitation of point tenderness over the greater trochanter, which reproduces the presenting symptoms. • Palpation may also reproduce pain that radiates down the lateral thigh.
Physical • Bursal swelling may be present, but this finding may be difficult to appreciate in many patients. • In obese patients, direct location of the trochanter may be difficult. Consider using the iliac crest as a landmark and assessing for the trochanter approximately 8 inches (20 cm) below the pelvic brim. Attempt to palpate the region while passively circumducting the affected hip.
Physical • Lateral hip pain can often be elicited with passive external rotation of the affected hip, whereas such symptoms are not provoked by internal rotation. External rotation can also be combined with passive hip abduction. • Lateral hip pain can also be reproduced with either passive hip adduction or active hip abduction.
Physical • If recent acute trauma has occurred, skin changes may include ecchymoses, abrasions, or both. • Groin pain produced through passive internal rotation of the hip may indicate hip joint pathology, such as osteoarthritis. • To assess for sciatica or lumbosacral radiculopathy, perform a careful neurologic examination in the bilateral lower limbs, including assessment of strength, reflexes, sensation, and dural stretch maneuvers (eg, straight-leg raise).
Causes • Acute trauma • A fall or tackle with the patient landing on the lateral hip region • Repetitive (cumulative) trauma • More common involvement than acute trauma • Caused when patients with tightness of the ITB run or even walk • Osteoarthritis of the hip, although this diagnosis generally manifests as groin or knee pain rather than lateral hip pain
Differentials • Femoral Head Avascular Necrosis • Femur Injuries and Fractures • Hip Fracture • IliopsoasTendinitis • IliotibialBand Syndrome • Lumbosacral Radiculopathy
Imaging Studies • If significant trauma is present, obtain radiographs of the hip and femur to assess for possible fracture(s). • If metastatic cancer is suspected (even in the setting of normal femur radiographic findings), a bone scan can be used to assess for lesions in the proximal femur. • MRI and ultrasonography (US) can potentially be used to differentiate between gluteus medius tendinitis and trochanteric bursitis (greater trochanteric pain syndrome, GTPS) in patients with GTPS.
Imaging Studies • A study performed by Blankenbaker et al reported all patients with trochanteric bursitis (greater trochanteric pain syndrome, GTPS) demonstrate peritrochanteric T2 abnormalities and have a higher incidence of abductor tendinopathy on MRI. However, MRI is a poor predictor of trochanteric bursitis (greater trochanteric pain syndrome, GTPS), because such findings are not specific for this pathology. • A study by Fearon et al concluded that ultrasound appears to be clinically useful in greater trochanteric pain syndrome (GTPS).[9]
Diagnostic injection of local anesthetic into the trochanteric bursa may be helpful, particularly in an obese individual in whom the diagnosis is not yet certain.
Complications • Chronic pain • Limited activity level • Limping (antalgic gait) • Sleep disturbance, which is especially problematic for patients who usually sleep on their sides
Rehabilitation • Management of the patient during the acute phase can include icing of the affected regions for 20-30 minutes every 2-3 hours. • The physical therapist can instruct the patient in a home exercise program, emphasizing stretching of the ITB and TFL and strengthening of the hip abductors, especially the gluteus medius. • The use of phonophoresis and soft-tissue massage may also be helpful. Transcutaneous electrical nerve stimulation (TENS) can be considered in cases that prove resistant to the rehabilitation program.
Rehabilitation • Stretching of the ITB and TFL can be achieved with a program that incorporates passive adduction of the knee of the affected limb across the midline as far as possible and maintenance of this position for at least 10-20 seconds. • This exercise can be repeated in various degrees of hip flexion, thus theoretically stretching the various ITB and TFL fibers. • To avoid exacerbation of trochanteric bursitis (greater trochanteric pain syndrome, GTPS) and/or its symptoms, stretching should not be performed in a ballistic, jerking fashion. Instead, stretches should be performed in a controlled and sustained fashion.
Rehabilitation • Sitting in and out of chairs. Direct pressure on the affected site should also be avoided. • Evaluation and correction of any underlying gait abnormalities are important and may be addressed with assistive devices (eg, cane, walker, orthotics, shoe lift, knee brace).
Rehabilitation • Use of deep-heating modalities (eg, US, TENS) should be considered in cases in which conventional therapy has failed
Surgical Intervention • Surgical intervention is generally not required for trochanteric bursitis (greater trochanteric pain syndrome, GTPS). • Patients with this condition rarely need a bursectomy and partial resection of the greater trochanteric process.
Other treatment • Corticosteroid injection into the trochanteric bursa • A mixture of a corticosteroid and a local anesthetic (eg, 40-80 mg of long-acting methylprednisolone [eg, Depo-Medrol; Pharmacia & Upjohn Co, Kalamazoo, Mich] and 5 mL of 1% lidocaine) can be injected into the affected trochanteric bursa with a 22-gauge needle. • A 1.5-inch (3.8-cm) needle may be adequate for a slim patient. A heavier patient may require a 3.5-inch (8.9-cm) needle to reach the bursa. • The needle is advanced to the greater trochanter and then is withdrawn slightly so that it is located within the bursa before the injection is made. • Further specifics of the injection procedure and potential complications are beyond the scope of this text. Interested clinicians are encouraged to read other appropriate sources.
Corticosteriod Injections • Lievense et al found that, depending on the treatment setting, the rates of corticosteroid injections were 34% for primary care, 37% for specialist, and 34% for hospital, resulting in improvement rates between 60% 1-year follow-up and 66% at 5-year follow-up. • Patients who had received a corticosteroid injection had a 2.7-fold higher chance of recovery after 5 years relative to those patients who had not received such an injection. Having had a corticosteroid injection was predictive for improvement within 5 years.
Medications • used primarily to decrease the pain and inflammation of trochanteric bursitis (greater trochanteric pain syndrome, GTPS • the most commonly used medications are oral nonsteroidal anti-inflammatory drugs (NSAIDs) and focal corticosteroid injections that are used in conjunction with the rehabilitation plan.