Download
1 / 25
411 likes | 1.57k Views
Exposure Options for Hip Revision: Trochanteric Osteotomies. Andrew Tice Arthroplasty Rounds April 12, 2012 Credit: Dr. Darwish and Dr. Hamdi. 4 Osteotomy Options. Transverse Trochanteric Osteotomy Trochanteric Slide Osteotomy Modified Trochanteric Slide Osteotomy

E N D
Exposure Options for Hip Revision:TrochantericOsteotomies Andrew Tice Arthroplasty Rounds April 12, 2012 Credit: Dr. Darwish and Dr. Hamdi
4 Osteotomy Options • Transverse TrochantericOsteotomy • Trochanteric Slide Osteotomy • Modified Trochanteric Slide Osteotomy • Extended TrochantericOsteotomy
Common Reasons for Hip Revision • Painful, aseptic loosening of one or both components • Infected total hip arthroplasty • Periprosthetic fracture • Recurrent or irreducible dislocations • Fracture or mechanical failure of implant • Progressive bone loss
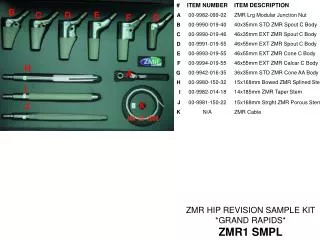
Preoperative Planning • Review of operative reports • X-ray analysis for type of prosthesis, amount of bone loss, templating • Equipment checklist may include: • Image intensifier and radiolucent OR table • Stem extraction instruments • Trephine reamers • Flexible osteotomes, curved osteotomes • Gigli saw • Metal-cutting instruments • Trochanteric fixation devices • Pelvic reconstruction screws/plates • Allograft bone (femoral head, struts, or segmental allograft)
Surgical Approaches • Consider previous incisions and possibility of skin necrosis • Less of a problem than in the knee • Anterolateral or direct lateral gluteal-splitting approaches used more commonly for straightforward acetabular revisions • Difficult exposure to posterior column of acetabulum as well as extensile exposure of the femur • Posterolateral approach • Excellent exposure of posterior column and femoral shaft • Anterior acetabular exposure is difficult • Greater risk of dislocation
TrochantericOsteotomies • Transverse Osteotomy • +++ Pelvic Exposure • + Femur Exposure • Trochanteric Slide • ++ Pelvic Exposure • ++Femur Exposure • Extended TrochantericOsteotomy • ++ Pelvic Exposure • +++ Femur Exposure
Transverse Osteotomy • Indications • Complex acetabular revisions • Antiprotrusio cage • Large structural acetabular bone graft • Recurrent dislocation with soft tissue laxity • Intrapelvic migration of acetabular component • Contraindications • Severe osteolysis with inadequate bone bed for reattachment • Advancement of trochanter more than 1 cm distally • Increases risk of non-union
Transverse Osteotomy • Technique • Vastuslateralis divided transversely and retracted distally • Gluteus minimum and medius bluntly elevated off capsule • Osteotomy performed with either oscillating saw, osteotome, or Gigli saw • Single plane osteotomy or Chevron biplane osteotomy • Fragment reflected proximally • Care not to stretch superior gluteal nerve • Fixation options: smooth wire, braided cables, plates plus wires
Transverse Osteotomy • Complications • Non union of the fragment and proximal migration • Rates quoted from 1 to 25% with average around 2-5% • Malunion • Painful Hardware • Persistent limp
Trochanteric Slide • Indications • Isolated acetabular revisions • AcetabuliProtrusio • Femoral revisions when maintaining the integrity of the diaphysis is a necessity • Contraindications • Absence of medial bone for reattachment • Insufficient trochanter thickness, with inadequate bed for repair
Trochanteric Slide • Technique • Similar to Transverse osteotomy, though vastuslateralis is not divided, just lifted distal to origin • Osteotomy from posterior to anterior starting between posterior borders of gluteus medius and minimus, and piriformis and short external rotators • AP width of osteotomy approximately 2 cm • Fragment retracted anteriorly • Reattachment with 2 or 3 double-loop cerclage wires
Trochanteric Slide • Complications • Non-Union • Similar rates as transverse osteotomy, though showed less superior migration more than 1 cm (11% of all nonunions) decreasing rate of abductor insufficiency and limp • Dislocation • Painful Hardware • Limp / Abduction Lurch (7%) • Malunion
Modified Trochanteric Slide • Uses Lateral approach to hip • Osteotomy only extended to 1 cm anterior to insertion of posterior capsule and external rotators • Goal is to reduce risk of dislocation by preserving the posterior structures (4% dislocation rate vs. 14% with standard trochanteric slide)
Extended TrochantericOsteotomy • Indications • Extraction of a well fixed femoral component • Difficult femoral cement removal • Varus remodeling of proximal femur • Avoid lateral cortex perforation • GT bony bed insufficient for healing other osteotomies • Aid in dislocation with extensive soft tissue scarring or HO • Contraindications • No intent of revising the femoral component • Revision with a cemented stem
Extended TrochantericOsteotomy • Technique • Most commonly posterolateral approach • Subperiosteal elevation of VastusLateralis and release of Gluteus Maximus • Osteotomy planned pre-op to at least the level of porous surface of implant, or further for cement mantle • Need to maintain at least 5 cm of isthmicdiaphyseal bone for fixation of new implant. Usually about 12-15 cm from GT
Extended TrochantericOsteotomy • Technique Continued • Osteotomy performed at may different times • Immediately to aid in dislocation, after dislocation, after stem extraction • Posterior to anterior cut • Then transverse cut is made at predetermined level • 1/3 diaphyseal circumference • Rounded corners reduce risk of iatrogenic fractures
Extended TrochantericOsteotomy • Technique Continued • Medial surface of the osteotomy frequently requires burring to accomodate the revision femoral component
Extended TrochantericOsteotomy • Retrospective review of 166 consecutive revision THA involving trochantericosteotomies • Nonunion rate of 1.2% • Mean time to union 12.3 weeks • 153 (92.1%) stems osseointegrated12 (7.2%) stems fibrous stable 1 (0.6%) stem unstable • Overall Complications rate (24%) and Revision Rate (10.2%)
Extended TrochantericOsteotomy • Nonunion: 1-3% • Fractures: 4-20% • Upward Migration of fragment: 0-1.2% • Infection: 1-3% • Subsidence of stem
References • Campbell’s Operative Orthopaedics. 11th ed. • Lakstein , D et al. Trochanteric Slide for Revision Total Hip Arthroplasty: Opening the Barn Door. SeminArthro 2011, 22:107-109. • Gross, A et al. Surgical Exposures for Primary and Revision Total Hip Arthroplasty: Modified Trochanteric Slide. SeminArthro 2004, 15:122-125. • Barrett, WP. Standard TrocantericOsteotomy. SeminArthro 2004, 15: 108-112. • Miner, TM et al. The Extended TrochantericOsteotomy in Revision Hip Arthroplasty. Journal of Arthroplasty 2001, 16:188-194. • Romero, AC et al. Sliding TrochantericOsteotomy Preserves Favorable Abductor Biomechanics in Revision Total Hip Arthroplasty. Journal of Arthroplasty 2001, 16: 55-64. • Mardones, R et al. Extended Femoral Osteotomy for Revision of Hip Arthroplasty. Journal of Arthroplasty 2005, 20: 79-83. • Goodman, S et al. Modified Sliding TrochantericOsteotomy in Revision Total Hip Arthroplasty. Journal of Arthroplasty 2004, 19: 1039-1041.

![READ [PDF] Stop Hip Bursitis Pain: Greater Trochanteric, Iliopsoas and Ischial Bursitis](https://cdn7.slideserve.com/12506317/slide1-dt.jpg)