Download
1 / 36
360 likes | 843 Views
NURSING AFTER SUNSET Violence & Aggression from a Night Shift Perspective. Mr. Joseph Galea RMN, RGN. B.Sc.(Hons.) Mental Health Nursing, BBA(Hons.) Business Administration, Cert. Subst. Misuse (UK) Departmental Nursing Manager - MCH MAPN Conference 2nd November 2012.

E N D
NURSING AFTER SUNSETViolence & Aggression from a Night Shift Perspective Mr. Joseph Galea RMN, RGN. B.Sc.(Hons.) Mental Health Nursing, BBA(Hons.) Business Administration, Cert. Subst. Misuse (UK) Departmental Nursing Manager - MCH MAPN Conference 2nd November 2012
1. Antecedents to Violence & Aggression 2. Night-Shift & Violence 3. Effects of Violence & Agression 4. Deescalation of a Crisis 5. Night-Shift 6. Effect of Night-Shift 7. Sleep Disorders & Fatigue 8. Under-reporting of Violence & Aggression Incidents 9. Recommendations Aims of the Presentation
Introduction (i) • Prevelance of violence in healthcare (Duncan et al., 2001; Gerberich et al., 2004; Lanza, Zeiss & Reirdan, 2006a) • Particularly on nursing staff (Findroff et al., 2004; Hodgson et al., 2004; Lanza, Zeiss & Reirdan, 2006b) • Impact on the physical & psychological health (Gerberich et al., 2004; Lanza, 1983, 1992; Lanza et al., 2006a; Woods & Ashley, 2007) • Impact on the ward environment and patients’ care (Flannery et al., 1995; Morrison, 1990)
Antecedents to Violence & Aggression (i) • Perpetrators of physical violence = patients (Acik et al., 2008; Chen et al., 2008) • Lateral violence = perpetrators of psychological violence = staff members, co-workers & supervisors (King & McInerney, 2006; Kwok et al., 2006; Johnson et al., 2007; Bigony et al., 2009) • Reasons for aggressive & violent behaviour – patients and nurses disagree – patients: environmental conditions + poor communication; nurses: patients’ mental illness (Duxbury & Whittington (2005) • Complex interactions of patients, staff and culture of a specific unit (Hamrin et al., 2009)
ANTECEDENTS to Violence and Aggression Medication Related Containment 2) Staff-Patient Interaction 1) Patient – Patient Interaction 8) Patient Symptoms Any other containment Any other staff-patient interaction Violence & Aggression 3) Patient Conflict Behaviors 5) Structural Issues Environmental Issues Regime Issues 7) Patient Emotional Cues 6) Patient Behavioral Cues 4) External / Personal Issues
Physical contact Intrusion into personal psychological or physical space (BAAEM, 2003; McPhauls & Lipscomb, 2008; May & Grubbs, 2002; Presley & Robinson, 2002) Competition Patient engaged in an activity Reaction to sexual approach Miscummunication Victim doing something patient wanted stopped Retaliation Patient victim characteristics Teased / bugged Provocation (Powell et al., 1994) Difference in language and culture (Mallet & Dougherty, 2000) Patient to Patient Interaction (Bowers et al. 2011)
Limiting patients’ freedom: (Sheridan et al., 1994; Lancee et al., 1995; Davis, 1991) and the limit style of nursing staff(Lancee et al., 1995; RCP, 2000) Medication related containment: a) medication administration, b) staff requesting patient to take medication, c) dispute over medication (Sheridan et al., 1990; Powell et al., 1994; Lancee et al., 1995; Davis, 1991) Any other containment: a) restraint, b) seclusion, c) de-escalation, d) ECT, e) involuntary admissions (Fineberg et al., 1990; Powell et al., 1994) Any othe staff-patient interaction: a) provocation. b) ordering patients, c) intervening on fight or argument, d) caring for patient, e) searching patients, f) negative staff attitude (OSHA, 2003; BAAEM, 2003), g) physical contact, h) patient engaged in an activity, i) miscommunication, j) staff too permissive, k) staff victim characteristics, l) staff errors, m) violation of priority (Mallet & Dougerty, 2000), n) lack of information(Mallet & Dougherty, 2000), o) access to staff(McGeorge et al., 2000). Staff-Patient Interaction (Bowers et al. 2011)
Patient conflict Behaviors(Bowers et al. 2011) : a) threatening behaviour, b) abscondments, c) substance misuse (BAAEM, 2003; Johnson, 1997), d) verbal agression, d) self-harm. External / Personal(Bowers et al. 2011) : a) money issues, b) visit from family member or friend(Henry & Ginn, 2002) (BAAEM, 2003), c) receiving bad news, d) unresolved family problem. Structural & Environmental issues(Bowers et al. 2011) : a) overcrowding (Fineberg et al., 1990; Palmstierna et al., 1991; Lanza et al., 1994), b) confined environment, c) noisy ward, d) patients found weapons, e) social environment such as boredom (RCP, 1998; RCP, 2000). Regime issues (Bowers et al. 2011): a) inadequate staffing levels (McPhaul & Lipscomb,2008; Gilmore-Hall, 2001, b) admitting / transferring / discharged & when pts ask to discharge themselves against medical advice (Sheridan et al., 1990;Powell et al., 1994; Lancee et al., 1995; Davis, 1991), c) excessive sensory stimulation, d) lack of stimulation. Patient Behavioral cues (Bowers et al. 2011): a) agitation, b) attention seeking behavior, c) increased motor activity, d) confusion. Patient emotional / mood cues (Bowers et al. 2011) : a) anger, b) sexual frustration, c) irritability, d) tobacco withdrawal, e) Delusions(Humphreys et al., 1992)& hallucinations (Dura, 1997),and stress due pain or illness (ICN, 2002; McPhauls & Lipscomb, 2008).
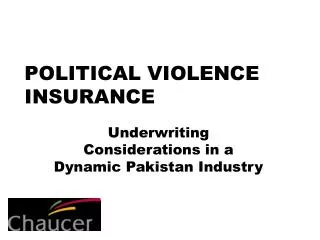
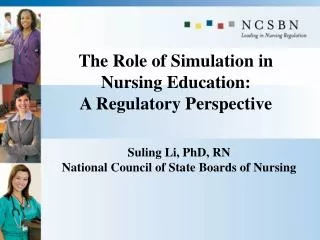
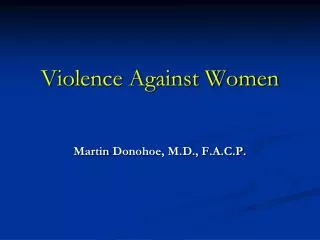
Night-Shift & Violence (i) • Violence experienced during night-shifts (Arnetz et al., 1996) particularly before 11pm. • Mostly occured during the afternoon – 3pm to 11pm (Bradley et al., 2001) – lack of structured interaction (Drinkwater, 1982; Rice et al., 1989) • There is no consensus. • Specific times for aggression: during admission – change of shifts – mealtimes (Pearson et al., 1986) – visiting hours (Way et al., 1992) – administration of medication (Walker & Siefert, 1994; Barnard et al., 1984; Depp, 1983).
Figure 1: Peak times for violent incidents FREQUENCY TIME Bowers et al., 2011
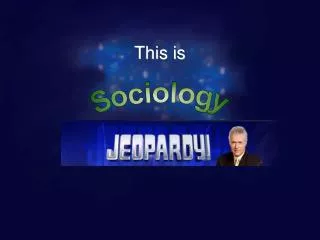
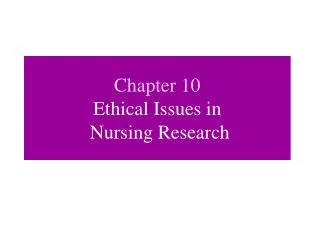
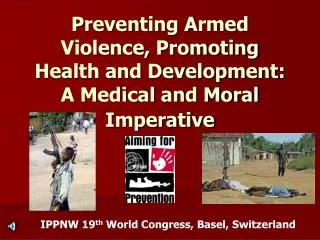
Night-Shift & Violence (ii) • Highest numbers of incident occurred between 7am – 3.30pm (morning shifts, 49% of the incidents); high number on afternoon shift (36%); during night (15%) (Barlow et al., 2000) • Aggression a daytime phenomenon (Barlow et al., 2000; Way et al., 1992; Shah et al., 1991) • Patients on leave – evening on return to the ward (Nobel & Rodger, 1989) • Preventing a patient leaving the ward (Walker & Siefert, 1994) • Staff uncertain of their roles (Katz & Kirkland, 1990) • Substitute nursing staff (James et al., 1990) • Higher staff to patient ratio(Morrison, 1990; Kalgerakis 1973; Depp, 1983) – more than 1:1 (Lanza et al., 1994)
FIG 1: Peak shifts for violent incidents FIG 2: Location of violent incidents FREQUENCY % SHIFT LOCATION Bowers et al., 2011
Staff – nurses (90% of incidents)(Edwards et al., 1988; Noble & Rodger, 1989) Patients (30%) were against patients(Noble & Rodger, 1989) Provoked by patients, relatives or visitors(Powell et al., 1994). Physical injuries(Chen et al., 2008) Psychological trauma(Chen et al., 2008) & PTSD (Caldwell, 1992; Mikkelsen & Einarsen, 2002; Hansen et al., 2006; Bigony et al., 2009) Negative impact on the mental health of nurses(Pai & Lee, 2011) Emotional reactions following violence include antipathy against perpetrator, insult and fear(Astrom et al., 2004) Negative organisational outcomes(Estryn-Behar et al., 2008; DHHS/NIOSH, 2002) Victims of in-patient violence Effects of Violence & Aggression
De-escalation of a Crisis • ‘Calming the patient’ – shift from a dominant-submissive connotation to collaboration (Richmond et al., 2012). • De-escalating a patient = form of a treatment = develop internal locus of control (Richmond et al., 2012). • This involves rapid assessment & decision-making skills
Good attitude Observation skills – verbal & non-verbal skills Risk Assessment skills Communication skills Listening skills (active listening) Active listening skills Emotional intelligence – self-monitoring Positive regard Empathic Quick decision making skills Assertiveness skills Team coordination skills Coaching skills Limit settings Motor skills Offer choices and optimism Restraining skills Debriefing skills Skills Needed (Richmond et al., 2012)
Night-Shift (i) • Work performed after 6pm and before 6am the next day. (Abdalkaber & Hayajneh, 2008) • Activity at night = out of phase with the circadian body temperature. = desynchronised state. (Abdalkaber & Hayajneh, 2008) • This disorientation = health & psychological effect of fatigue. (Abdalkaber & Hayajneh, 2008)
What these three sets of pictures have in common?(Rogers et al., 1997; Harrington, 2001)
Night-Shift (ii) • To ensure patient’s coverage nurses have to work nights, weekends and holidays. • Night nurses have higher levels of fatigue (Muecke, 2005) and mental tiredness (Tepas et al., 2004), chronic sleep loss, sleep deprivation and on-the-job sleepiness (Hughes & Stone, 2004). • Rarely get the recommended 8 hrs of sleep (Akerstedt, 2003). • Suffer from sleep disturbances (Barton, 1994) – which may have an impact on patients’ safety. • Less quality sleep then those working during the day (Ruggiero, 2003; Frank & Ovens, 2002). • Sleep deprivaton – work performance outcomes – safety and general health of the nurse (Rogers et al., 2004)
Night-Shift (iii) • The 2nd half of the night is where nurses reported that they frequently struggle to stay awake (Berger & Hobbs, 2006). • Staff’s circadian rhythm – social – family life – general health affected (Rosa & Collingan, 1997). • Nurse who work nights are more depressed than day nurses (Ruggiero, 2003) / there is an association between night work and poor job satisfaction (Korompeli et al., 2009). • Staff performance: Significant associations between night staff and error rate (Gold et al., 1992; Leff et al., 2008).
Effects of Night-Shifts • Two things wrong with shift-work: • Having to work when supposed to sleep • Having to sleep when supposed to be awake • For some people, this can result in performance, health and social effects • Fatigue = less work performance + short staffing = less the quality of patient care (Circadian Technologies, 2004) • Breast Cancer to be 60% higher in women night-shift workers (Humm, 2005; Swerdlow, 2003; Steven & Davis, 1996) infertility, cardiovascular disease, diabetes and gastrointestinal disorders (Humm, 2005; Reid et al., 1997; Learhart, 2000). • Fatigue, irritability (Lushington et al., 1997; Reid et al., 1997), reduced performance, decreased mental agility (Alward & Monk, 2003).
Circadian Rhythms • Fatigue = impair memory, vigilance, reaction time, and communication = cyclic reductions in alertness and performance (Howard et al., 2002). • Internal body clock – external world (zeitgebers) • High activity during the day – low activity during the night • Human race is diurnal • Health problems (Crofts, 1999), negative effects: for the individual & the work place – decreased alertness & reduced job performance – affect the quality of care (Koller, 1996; Brown & Erkes, 1998) • Optimum mental performance level (2-4pm) and maximum general awareness is between (1-7pm. Performance levels are lowest between 3.30 – 5.30am (Coffey et al., 1998)
Sleep Disorders (i) • Lack of sleep (Coffey et al., 1998) • Sleep disorder – tiredness – reduced functional capacity • Functional capacity may be halved after 24 hrs and after 48 hrs is at its lowest • Complex decisions (Akerstedt, 1999) though short term memory recall is not effected (Allen, 1999) • Sleep deprivation – disrupt the circadian rhythm – forces the body to function at night despite signals (i.e. Decreased body temp. & increased melatonin (Hughes & Stone, 2004)
Sleep Disorders (ii) • Sleep quantity and sleep quality affected especially with night work • Daytime sleep not as deep or refreshing • Worse when room is not quite, not dark and not comfortable • Sleep quantity: Night shift (4-6 hrs) – Day shift (7.5 hrs) – Evening (8.5 hrs) • Sleep quality: day sleep – less deep sleep (stage 3 – 4); Rotating shift < Permanent shift • Sleep deprivation of 24 hours affect performance level (blood alcohol levels of 0.10%) (Dawson & Reid, 1997). Mature vs young night shift workers (Reid & Dawson, 2001).
Night shift related fatigue and sleep difficulties (Bonnet, 2000; Harrison & Horne, 2000) Negative mood Sleep loss and fatigue Lack of innovation and creativity Increased distractability Inability to deal with unexpected events Inability to deviate from previous problem-solving strategies Unreliable temporal memory Impaired language skills Motor skill performance can be impaired (Eastridge et al., 2003; Grantcharov et al., 2001) Skill error increase (Taffinder et al., 1998) Skills required when dealing with violence & aggression Good attitude Observation skills – verbal & non-verbal skills Risk Assessment skills Communication skills Listening skills (active listening) Active listening skills Emotional intelligence – self-monitoring Positive regard Quick and empathic decision making skills Assertiveness skills Team coordination skills Coaching skills Limit settings Motor skills Offer choices and optimism Restraining skills Debriefing skills The Combination of Night Shift Nursing with Aggression & Violence
Under-Reporting of Violence • Insufficient post-incident support(Pai & Lee, 2011; Kwok et al., 2006; Kamchuchat et al., 2008) • Stigma of victimisation(Hoff, 1992) • Accepted as a hazard of the profession(Daldt, 1981); part of the job (Poster, 1996; Prins, 1999) • Resistance from hospital administrators(Lanza, 1991) • Peer nursing pressure(Kinross, 1992) • Poor or ineffective reporting mechanisms (Lyon et al., 1981; Pearson et al., 1986; Silver & Yudofsky, 1987; Lanza, 1988; Monahan, 1989) • Lack of support from organisation (Paterson et al., 1999)but staff wassupported by their immediate nursing colleagues(McGeorge et al., 2000) • Lack of institutional reporting policies, employees beliefs and concerns (Sofiel & Salmond, 2005); Ferns, 2005; May & Grubbs, 2002, US Dept of Labor, 2008)
Recommendations • Managment awareness – planning shift schedules – aware of biological rhythms. • Regular medical screening & breast screeing for night female nurses over 40 years of age • For health reasons – option to day work – option to night work • Critical incident stress debriefing or therapy • Training & Re-organisation of the ward routine (McGeorge et al., 2000) • Increasing face-to-face contact • Improving information sharing • Interaction with staff and patients • A significant amount of workplace aggression is preventable (DelBel, 2003). Education programs for nurses on fatigue and night work (Circadian Techologies, 2004) • Violence prevention programs (Kindy, 2005; Anderson & Parish, 2003; Gilmore-Hall, 2001; McPhaul & Lipscomb, 2008; US Dept of Labor, 2008)
Conclusion • Link = human interaction & violence • Less incidents during the night – atmosphere tend to be more quiter • The organisation of ward routine • Staff-patient interaction = associated with violence • Good practioner during day not necessarily mean good practitioner during the night.
Final thought...... ‘THE BEST FIGHTER IS NEVER ANGRY’ ................ Lao Tzu ‘but never tired ’.......
References Abdalkader, R. H., & Hayajneh, F. A. (2008). Effect of Night Shift on Nurses Working in Intensive Care Units at Jordan University Hospital. European Journal of scientific Research, 23 (1), 70-86. Acik, Y., Deveci, S. F., Gunes, G., Gulbayrak, C., Dabak, S., Saka, G., Vural, G., Can, G., Bilgin, N. G., Dundar, P, E., Erguder, T., & Tokdemir, M. (2008). Experience of workplace violence during medical speciality training in Turkey. Occupational Medicine 58, 361-366. Akerstedt, T. (1996). Subjective and objective sleepiness in the active individual. International Journal of NeuroScience, 52, 29-37. Allen, C. (1999). Summary of the Croet Seminar: Shift work. Retrieved from http://www.ohsu.edu/Croet/outreach/symposia/shiftwork.html. Accessed on 10.03.04. Anderson, C., & Parish, M. (2003). Report of workplace violence by Hispanic nurses. J Transcult Nurs. 14, 237-243. Alward, R., & Monk, T. (1993). The Nurse’s Shift Work Handbook. Washington DC: American Nurses Publishing. Arkestedt, T. (2003). Shift work and disturbed sleep/wakefulness. Occupational Medicine, 53, 89-94. Arnetz, J. E., & Arnetz, B. B., & Petterson, I. L. (1996). Violence in the nursing profession: occupational and life stule risk factos in Swedish nurses. Work and Stress, 10, 119-127. Astrom, S., Karlsson, S., & Sandvide, A. (2004). Staff’s experience of and the management of violent incidents in elderly care. Scand J Caring Science, 18, 157-161. Barlow, K., Grenyer, B., & Ilkiw-Lavalle, O. (2000). Prevalence and precipitants of aggression in psychiatric inpatients unit. Australian and New Zealand Journal of Psychiatry, 34, 967-974. Barnard, G., Robbins, L., & Newman, G. (1984). A study of violence within a forensic treatment facility. Bulletin of the American Academy of Psychiatry and the Law, 12, 339-348. Barton, J. (1994). Choosing to work at night: a moderating influence of individual tolerance to shift work. Journal of Applied Psychology, 79 (3), 449-454. Berger, A., & Hobbs, B. (2006). Impact of shift work on the health and safety of nurses and patients. Clinical Journal of Oncology Nursing, 10 (4), 465-470. Bigony, L., Lipke, T. G., Lundberg, A., McGraw, C. A., Pagae, G. L., & Rogers, A. (2009). Lateral violence in the perioperative setting. AORN Journal, 89, 688-700. Bonnet, M H. (2000). Sleep deprivation. In M. H., Kryger, , T. Roth, & W. C. Dement (Ed.), Principles and practive of sleep medicine (3rd ed., pp. 53-71). Philadedelphia: W. B. Saunders. Bowers. L., Stewart, D., Papadopoulos, C., Duck, C., Ross, J., Khanom, H., & Jeffery, D. (2011). Inpatient vilence and aggression: a literature review. Institute of psychiatry, King’s College London. British Association for Accident and Emergency Medicine. Violence in Accident and Emergency Departments. Notes of Guidance. Retrieved from http://www.baem.org.uk. Accessed on 3/3/03. Brown, A. (1998). Turning Body Times to Shift Time. Health Science Centre, 94, 51-52.
Caldwell, M. F. (1992). Incidence of PTSD amond staff victims of patient violence. Hospital Community Psychiatry, 43, 838-839. Chen, W. C., Hwu, H. G., Kung, S. M., Chiu, H. J., & Wang, J. D. (2008). Prevalence and determinants of workplace violence of health care workers in a psychiatric hospital in Taiwan. Journal of Occupational Health, 50, 288-293. Circadian Technologies Inc. (2004). Human Resources Management in the Extended Hourse Workplace. Retrieved from http://www.circadian.com/publications/nursing.html. Accessed on 14.09.2005. Coffey, l., Skipper, J., & Jung, F. (1998). Nurses and Shift Work Effect on Job Performance and Job Related Stress. Journal of Advanced Nursing, 13 (2), 245-254. Crofts, L. (1999). Challenging shift work: A review of common rostering practices in UK Hospitals. Nursing Progress, 9 (30), 36-56. Daldt, B. W. (1981). Anger: an alienation communication bazard for nurses. Nursing Outlook, 29, 640-644. Davis, S. (1991). Violence by psychiatric inpatients: a review. Hospital and Community Psychiatry, 42, 585-590. Dawson, D., & Reid, K. (1997). Fatigue, alcohol and performance impairment. Nature, 388 (6639), 235. DelBel, J. C. (2003). Deescalating workplace aggression. Nurs Mange, 34 (9), 30-34. Depp, F. C. (1983). Assualts in public mental hospital, in Assualts Within Psychiatric Facilities. Edited by Lino, J. R., & Reid, W. H. New York, Grune & Stratton. DHHS/NIOSH. (2002). Violence: Occupational Hazards in Hospitals. National Institute for Occupational Safety and Health, Washington, DC. Drinkwater, J. (1982). Violence in psychiatric hospitals, in Developments in the Study of Clinical Behavior, vol. 2: Violence. Edited by Feldman P. Chichester, Wiley. Duncan, S. M., Hyndman, K., Estabrooks, C. A. Hesketh, K., Humphrey, C. K., Wong, J. S., et al. (2001). Nurses’ experience of violence in Aloberta and British Columbia hospitals. Canadian Journal of Nursing Research, 32, 57-78. Dura, J. (1997). Expressive communicative ability, symptoms of mental illness and aggressive behavior. Journal of Clinical Psychology, 53, 307-318. Duxbury, J., Whittington, R. (2005). Causes and management of patient aggression and violence: staff and patient perspectives. Journal of Advanced Nursing, 50 (5), 469-478. Eastridge, B. J., Hamilton, E. C., O’Keefe, G. E., Rege, R. V., Valentine, R. J., Jones, D. J., et al., (2003). Effect of sleep deprivation on the performance of simulated laparoscopic surgical skills. American Journal of Surgery, 186, 169-174. Edwards, J. G., Jones, D., Reid, W. H., & Chu, C. C. (1988). Physical assualts in a psychiatric unit of a general hospital. American Journal of Psychiatry, 145, 1568-1571. Estryn-Behar, M., van der Heijden, B., Camerino, D., Fry, C., Le Nezet, O., Conway, P. M., & Hasselhron, H. (2008). Occupational Medicine, 58, 107-114.
Ferns, T. (2005). Violence in the accident and emergency department: an international perspective. Accid Emerg Nurs, 13, 180-185. Frank, J., & Ovens, H. (2002). Shiftwork and emergency medical practice. Can J. Emerg Med. 4 (6), 421-436. Findroff, M. J., McGovern, P. M., Rozman, J. M., & Gerberich, S. G. (2000). The cost of violence to healthcare workers. Journal of Healthcare Safety: Compliance and Infection Control, 4, 209-217. Flannery, R. B., Hanson, M. A., Penk, W. E., Goldfinger, S., Pastva, G. J., & Navon, M. A. (1998). Replicated declines in assualt rates after implementation of the assualted staff action program. Psychiatric Services, 49, 241-243. Gerberich, S. G., Church, T. R., McGovern, P. M., Hansen, H. E., Nachreiner, N. M., Geisser, M. S., et al., (2004). An epidemiological study of the magnitude and consequences of work related violence: The Minnesota Nurses’ Study. Occupational and Environmental Medicine, 61, 495-503. Gilmore-Hall, A. (2001). Violence in the workplace: are you prepared? Am J Nursing, 101 (7), 55-56. Gold, D., R. Rogacz, S., Bock, N., Tosteson, T. D., Baum, T. M., & Spezer, F. E. (1992). Rotating shift work, sleep and accidents related to sleepiness in hospital nurses. American Journal of Public Health, 82 (7), 1011-1014. Grantcharov, T. P., & Bardram, L., Funch-Jensen, P., & Rosenberg, J. (2001). Laparoscopic performance after one night on call in a surgical department: Prospective study. British Medical Journal, 323, 1222-1223. Hansen, A. M., Hogh, A., Persson, R., Karlson, B., Garde, A. H., & Orbaek, P. (2006). Bullying at work, health outocmes and physiological stress response. Journal of Psychosomatic Research, 60, 73-72. Hamrin, V., Iennaco, J., Olsen, D. (2009). A review of ecologival factors affectng inpatient psychiatric unit violence: implication for relational and unit cultural improvements. Issues in Mental Health Nursing, 30 (4), 214-226. Harrington, J. (2001). Health effects of shift work and extended hours of work. Occupational and Environmental Medicine, 58 (1), 68-72. Harrison, Y., & Horne, J. A. (2000). The impact of sleep deprivation on decision making: A review. Journal of Experimental Psychology: Applied, 6, 236-249. Henry, J., & Ginn, G. Violence prevention in healtcare organisations within a total quality management framework. Journal of Nursing Administration 32, (9), 479-86. Hodgson, M. J., Reed, R., Craig, T., Murphy, F., Lehmann, L., Belton, L, et al., (2004). Violence in healthcare facilities: Lessons from the Veterans Health Administration. Journal of Occupational and Environmental Medicine, 46, 1158-1165.
Hoff, L. A. (1992). Batterred women. Understanding, identification, and assessment – a psychosociocultural perspective. Journal of Advanced Nursing, 20, 627-634. Howard, S., Rosekind, M., Katz, J., & Berry, A. (2002). Fatigue in anaesathesia: implications and strategies for patient and provider safety. Anesthesiology, 97 (5), 1281-1294. Hughes, R., & Stone, P. (2004). The perils of shift work – evening shift, night shift, and rotating shifts: are they fit for you? Am J Nurs., 104 (9), 60-63. Humm, C. (2005). In the dark. Nursing Standards, 19 (24), 20-21. Humphreys, M. S., Johnstone, E. C., macMillan, J. E., & Taylor, P. J. (1992). Dangerous behavior preceding first admission for shcizophrenia. British Journal of Psychiatry, 161, 501-505. Infantino, J. A. J., & Musingo, S. (1985). Assualts and injuries among staff with and without training in aggression control techniques. Hospital and Community Psychiatry, 36, 1312-1314. International Council of Nurses. Wokplace violence in the health sector. Retrieved from http://www.icn.ch/images/stories/documents/pillars/sew/sew_workplace_violence_in_the_health_sector_state_of_the_art_paper.pdf Accessed on 01.10.12 James, D. V., Fineberg, N. A., & Shah, A. K. (1990). An increase in violence on an acute psychiatric ward: a study of associated factors. British Journal of Psychiatry, 156, 846-852. Johnson, C., Maritn, S., & Markle-Elder, S. (2007). Stopping verbal abuse in the workplace. The American Journal of Nursing, 107, 32-34. Johnson, S. (1997). Dual diagnosis of sever mental illness and substance misuse: a case for specialist services? British Journal of Psychiatry, 171, 205-208. Kalogerakis, M. G. (1973). The assualtive psychiatric patient. Psychiatric Quaterly, 45, 372-381. Kamachuchat, C., Chongsuvivatwong, V., Oncheunjit, S., Yip, T. W., & Sangthong, R. (2008). Workplace violence directed at nursing staff at a general hospital in southern Thailand. Journal of Occupational Health, 50, 201-207. Katz, P.,, & Kirkland, F. R. (1990). Violence and social structure on mental hospital wards. Psychiatry, 53, 262-277. Kindy, D., Peterson, S., Parkhurst, D. (2005). Perilous work: nurses’ experiences in psychiatric units with high risk of assualt. Archives of Psychiatric Nursing, 19 (4), 169-175. King, L. A., & McInerney, P. A. (2006). Hospital workplace experiences of registered nurses that have contributed to their resignation in the Durban metropolitan area. Curationis, 29, 70-81.
Kinross, l. (1992). Nurse assualt: overcoming the barriers to prevention. The Nursing Report. Canadian Nursing Management (Supplement) 49, 4-8. Kok, R. P. W., Law, Y. K., Li, K. E., Ng, Y. C., Cheung, M. H., Fung, V. K. P., Tong, J. M. K., Yen, P. F., & Leung, W. C. (2006). Prevalencce of workplace violence against nurses in Hong Kong. Hong Kong Medical Journal, 12, 6-9. Koller, M. (1996). Occupational Health Services for Shift and Night Workers. Applied Ergonomics, 27 (1), 31-37. Korompeli, A., Sourtzi, P., Tzavara, C., & Velonakis, E. (2009). Rotating shift-related changes in hormone levels in intensive care unit nurses. Journal of Advanced Nursing, 65 (6), 1274-1282. Lancee, W. J., Gallop, R., McCay, E., & Toner, B. (1995). The relationship between nurses’ limit setting styles and anger in psychiatric inpatients. Psychiatric Services, 46, 409-613. Lanza, M. L. (1983). The reactions of nursing staff to physical assualt by a patient. Hospital and Community Psychiatry, 34, 44-47. Lanza, M. L. (1988). Factors relevant to patient assualt. Issues in Mental Health Nursing, 9, 239-258. Lanza, M. L. (1991). Patient assualts: a comparison study of reporting methods. Journal of Nursing Quarterly Assurance, 5, 60-68. Lanza, M. L. (1992). Nurses as patient assualt victimsL An update, synthesis and recommendations. Archives of Psychiatric Nursing, 6, 163-171. Lanza, M. L., Kayne, H. L., & Hicks, C. (1994). Environmental characteristics realted to patient assualt. Issues in Mental Health Nursing, 15, 319-335. Lanza, M., Zeiss, R., & Rierdan, J. (2006a). Violence against psychiatric nurses: Sensitive research as science and intervention. Contemporary Nurse, 21, 71-84. Lanza, M., Zeiss, R., & Rierdan, J. (2006b). Non-physical violence: A risk factor for physical violence in healthcare settings. American Association of Occupational health Nursing Journal, 54, 397-402. Lanza, M. L., Rierdan, M. F. A., Forester, L., & Zeiss, R . (2009). Reducing Violence Against Nurses: The Violence Prevention Community Meeting. Issues in Mental Health Nursing, 30, 745-750. Leahart, S. (2000). Health effects of internal rotation of shifts. Nursing Standard 14, (47), 34-36.
Lee, S. S., Gerberick, S. G., Waller, L. A., Anderson, A., & McGovern, P. (1999). Work-related assualt injuries among nurses. Epidemiology, 10, 685-691. Leff, D. R., Aggarwal, R., Rana, M., Nakhjavani, B., Purkayastha, S., Khullar, V. et al. (2008). Laparoscopic skills suffer on the first shift of sequential night shifts: program directors beware and residents prepare. Annals of Surgery, 247 (3), 530-539. Lehmann, L. S., McCormack, R., A., & Kizer, K. W. (1999). A survey of assualtive behaviour in Veteran Health Administration facilities. Lushington, W., Lushington, K., & Dawson, D. (1997). The percieved social and domestic consequences of shiftwork for femal shift-workers (nurses) and their partners. Journal of Occupational Health and Safety-Australia and New Zealand, 13, (5), 461-469. Lyon, J. R., Snyder, W. & Merrill, G. (1981). Undereporting of assualts on staff in a state hospital. Hospital and Community Psychiatry, 32, 497-498. Mallett, J., & Dougherty, L., (2000). The Royal Marsden Manual of Clinical Nursing Procedures, (5th ed.). Blackwell Science. May, D. D., & Grubbs, L. (2002). The extent, nature, and precipitating factors of nurse assault among three groups of registered nurses in a regional medical center. J Emerg Nurs, 28 (1), 11-17. McPhaul, K. M., & Lipscomb, J. A. Workplace violence in healthcare: recognised but not regulated. Online J Issues Nurs. 2004;9. Available at http://www.nursingworld.org/MainMenuCategories/ANAMarketplace/ANAPeriodicals/OJIN/TableofContents/Volume92004/No3Sept04/ViolenceinHealthCare.html. Accessed on 01.10.12 Mikkelsen, E. G., & Einarsen, S, (2002). Basic assumptions and symptoms of post-traumatic stress among victims of bullying at work. European Journal of Work and Organisational Psychology, 11, 87-111. Monahan, J. (1989). Predicting Violence among the mentally Ill (sound cassette). Audio Digest-Psychiatry. Morrison, E. F. (1990). The tradition of toughness. Image: Journal of Nursing Scholarship, 22, 32-38. Morrison, E. F. (1990). Violent psychiatric inpatients in a public hospital. Scholarly Inquiry for Nursing Practice: An International Journal, 4, 65-82. Mueckem S. (2005). Effects of rotating night shifts: literature review. Journal of Advanced Nursing, 50 (4), 433-9. Noble, P., & Rodger, S. (1989). Violence by psychiatric in-patients. British Journal of Psychiatry, 155, 384-390. Pai, H. C., & Lee, S. (2011). Risk factors for workplace in clinical registered nurses in Taiwan. Journal of Clinical Nursing, 20, 1405-1412. Palmstierna, T., Huitfeldt, B., & Wistedt, B. (1991). The relationship of crowding and aggressive behavior on a psychaitric intensive care unit. Hospital and Community Psychiatry, 42, 1237-1240. Pearson, M., Wilmont, E., & Padi, A. (1986). A study of violent behavior among in-patients in a psychiatric hospital. Journal of Psychiatry, 149, 232-235.
Powell, G., Caan, W., & Crowe, M. (1994). What events precede violent incidents in psychiatric hospitals? British Journal of Psychiatry, 165, 107-112. Presley, D. & Robinson, G. (2002. Violence in the emergency department: nurses contend with prevention in the healthcare arena. Nurs Clin North Am, 37 (1), 161-169. Reid, K., Roberts, T., & Dawson, D. (1997). Imrpving shiftwork management ii:shiftwork and health. Journal of Occupational Health and Safety-Australia and New Zealand, 13, (5), 439-450. Reid, K., & Dawson, D. (2001). Comparing performance on a simulated 12 hour shift rotation in youn and older subjects. Occupational and Environmental Medicine, 58 (1), 58-62. Richmond, J. S., Berlin, J. S., Fishkind, A, B., Holloman, G. H., Zeller, S, L., Wilson, M. P., Rifia, M. A., & Ng, A. T. (2012). Verbal De-escallation of the Agitated Patient: Consensus statement of the American Association for Emergency Psychiatry Project BETA De-escallation Workgroup. Western Journal of Emergency Medicine, VolXIII, no. 1, 17-25. Rice, M. E., Harris, G. T., & Varney, G. W. (1989). Violence in Institutions. Toronto, Hogrefe & Huber. Rosa, R. R., & Colligan, M. J. (1997). Plain Language About Shiftwork. US Department of health and Human Services Public Health Service, Centers for Disease and Prevention. Cincinnati. Rogers, N., Roberts, T., & Dawson, D. (1997). Improving shift work management 1: understanding shiftwork. Journal of Occupational Health and Safety-Australia and new Zealand, 13 (5), 429-437. Rogers, A. E., Hwang, W., Scott, L. D., Arken, L. H., & Dubges, D. F. (2004). The working hours of hospital staff nurses and patient safety. Health Affairs (Millwood, Va.) 23, (4), 202-212. Ruggiero, J. S. (2003). Correlates of fatigue in critical care nurses. Research in Nursing & Health, 26 (6), 434-444. Shah, A. K., Fineberg, N. A., & James, D. V. (1991). Violence among psychiatric inpatients. Acta Psychiatrica Scandinavica, 84, 305-309. Silver, J. M., & Yodofsky, S. C. (1987). Documentation of aggression in the assessment of the violent patient. Psychiatric Annals, 17, 375-384. Sheridan, M., Henrion, R. E., Robinson, L., Baxter, V. (1990). Precipitants of violence in a psychiatric inpatient setting. Hospital and Community Psychiatry, 41, 776-780. Sofield, L., & Salmond, S. W. (2003). A focus on verbal abuse and intent to leave the organisation. Orthop Nurs. 22 (4), 274-283. Stevens, R. G., & Davis, S. (1996). The melatonin hypothesis: eclectic power and breast cancer. Environmental Health Perspective, 104, (1), 135-140. Swerdlow, A. (2003). Shift work and breast cancer: a critical review of the Epidemiological Evidence. Norwich: Her majesty’s Stationery Office, Health and Safety Executive. Retrieved from www.hse.gov.uk/research/rrpdf/rr132.pdf. Accessed on 10.10.12 Tepas, D. I., Barnes-Farrell, J. L., Bobko, N., Fischer, F. M., Iskra-Golec, I., & Kaliterna, L. (2004). The impact of night work on subjective reprots of well-being: an exploratory study of health care workers from five nations. Rev Saude Publica (Journal of Public Health), 38 (supplement), 26-31. US Department of Labor, Occupational Safety and Health Administration. (2004). Guidelines for preventing workplace violence for health care & social workers. Retrieved from http://www.osha.gov/Publications/OSHA3148.html#test1. Accessed on 07.01.08. US Department of Justice Federal Bureau of Investigation. (2004). Workplace violence: issues in response. Retrieved from http://www.fbi.gov/publications/violence.pdf. Accessed on 07.01.08 Walker, Z. & Seifert, R. (1994). Violent incidents in a psychiatric intensive care unit. British Journal of Psychiatry, 164, 826-828. Way, B. B., Braff, J. L., Hafemeister, T. L., & Banks, S. M. (1992). The relationship between patient-staff ratio and reported patient incidents. Hospital and Community Psychiatry, 43, 361-365. Woods, P., & Ashley, C. (2007). Violence and aggression: a literature review. Journal of Psychiatric and Mental Health Nursing, 14 (7), 652-660.