Download
1 / 1
40 likes | 143 Views
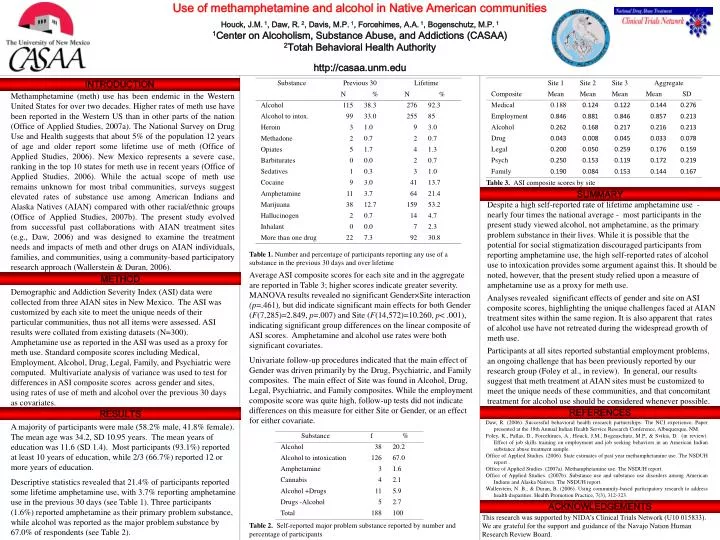
Use of methamphetamine and alcohol in Native American communities Houck, J.M. 1 , Daw, R. 2 , Davis, M.P. 1 , Forcehimes, A.A. 1 , Bogenschutz, M.P. 1 1 Center on Alcoholism, Substance Abuse, and Addictions (CASAA) 2 Totah Behavioral Health Authority http://casaa.unm.edu. INTRODUCTION.

E N D
Use of methamphetamine and alcohol in Native American communities Houck, J.M. 1, Daw, R. 2, Davis, M.P. 1, Forcehimes, A.A. 1, Bogenschutz, M.P. 1 1Center on Alcoholism, Substance Abuse, and Addictions (CASAA) 2Totah Behavioral Health Authority http://casaa.unm.edu INTRODUCTION Methamphetamine (meth) use has been endemic in the Western United States for over two decades. Higher rates of meth use have been reported in the Western US than in other parts of the nation (Office of Applied Studies, 2007a). The National Survey on Drug Use and Health suggests that about 5% of the population 12 years of age and older report some lifetime use of meth (Office of Applied Studies, 2006). New Mexico represents a severe case, ranking in the top 10 states for meth use in recent years (Office of Applied Studies, 2006). While the actual scope of meth use remains unknown for most tribal communities, surveys suggest elevated rates of substance use among American Indians and Alaska Natives (AIAN) compared with other racial/ethnic groups (Office of Applied Studies, 2007b). The present study evolved from successful past collaborations with AIAN treatment sites (e.g., Daw, 2006) and was designed to examine the treatment needs and impacts of meth and other drugs on AIAN individuals, families, and communities, using a community-based participatory research approach (Wallerstein & Duran, 2006). Table 3. ASI composite scores by site SUMMARY Despite a high self-reported rate of lifetime amphetamine use - nearly four times the national average - most participants in the present study viewed alcohol, not amphetamine, as the primary problem substance in their lives. While it is possible that the potential for social stigmatization discouraged participants from reporting amphetamine use, the high self-reported rates of alcohol use to intoxication provides some argument against this. It should be noted, however, that the present study relied upon a measure of amphetamine use as a proxy for meth use. Analyses revealed significant effects of gender and site on ASI composite scores, highlighting the unique challenges faced at AIAN treatment sites within the same region. It is also apparent that rates of alcohol use have not retreated during the widespread growth of meth use. Participants at all sites reported substantial employment problems, an ongoing challenge that has been previously reported by our research group (Foley et al., in review). In general, our results suggest that meth treatment at AIAN sites must be customized to meet the unique needs of these communities, and that concomitant treatment for alcohol use should be considered whenever possible. Table 1. Number and percentage of participants reporting any use of a substance in the previous 30 days and over lifetime Average ASI composite scores for each site and in the aggregate are reported in Table 3; higher scores indicate greater severity. MANOVA results revealed no significant Gender×Site interaction (p=.461), but did indicate significant main effects for both Gender (F(7,285)=2.849, p=.007) and Site (F(14,572)=10.260, p< .001), indicating significant group differences on the linear composite of ASI scores. Amphetamine and alcohol use rates were both significant covariates. Univariate follow-up procedures indicated that the main effect of Gender was driven primarily by the Drug, Psychiatric, and Family composites. The main effect of Site was found in Alcohol, Drug, Legal, Psychiatric, and Family composites. While the employment composite score was quite high, follow-up tests did not indicate differences on this measure for either Site or Gender, or an effect for either covariate. METHOD Demographic and Addiction Severity Index (ASI) data were collected from three AIAN sites in New Mexico. The ASI was customized by each site to meet the unique needs of their particular communities, thus not all items were assessed. ASI results were collated from existing datasets (N=300). Amphetamine use as reported in the ASI was used as a proxy for meth use. Standard composite scores including Medical, Employment, Alcohol, Drug, Legal, Family, and Psychiatric were computed. Multivariate analysis of variance was used to test for differences in ASI composite scores across gender and sites, using rates of use of meth and alcohol over the previous 30 days as covariates. REFERENCES RESULTS Daw, R. (2006). Successful behavioral health research partnerships: The NCI experience. Paper presented at the 18th Annual Indian Health Service Research Conference, Albuquerque, NM. Foley, K., Pallas, D., Forcehimes, A., Houck, J.M., Bogenschutz, M.P., & Svikis, D. (in review). Effect of job skills training on employment and job seeking behaviors in an American Indian substance abuse treatment sample. Office of Applied Studies. (2006). State estimates of past year methamphetamine use. The NSDUH report . Office of Applied Studies. (2007a). Methamphetamine use. The NSDUH report. Office of Applied Studies. (2007b). Substance use and substance use disorders among American Indians and Alaska Natives. The NSDUH report. Wallerstein, N. B., & Duran, B. (2006). Using community-based participatory research to address health disparities. Health Promotion Practice, 7(3), 312-323. A majority of participants were male (58.2% male, 41.8% female). The mean age was 34.2, SD 10.95 years. The mean years of education was 11.6 (SD 1.4). Most participants (93.1%) reported at least 10 years of education, while 2/3 (66.7%) reported 12 or more years of education. Descriptive statistics revealed that 21.4% of participants reported some lifetime amphetamine use, with 3.7% reporting amphetamine use in the previous 30 days (see Table 1). Three participants (1.6%) reported amphetamine as their primary problem substance, while alcohol was reported as the major problem substance by 67.0% of respondents (see Table 2). ACKNOWLEDGEMENTS This research was supported by NIDA’s Clinical Trials Network (U10 015833). We are grateful for the support and guidance of the Navajo Nation Human Research Review Board. Table 2. Self-reported major problem substance reported by number and percentage of participants