Download
1 / 1
10 likes | 89 Views
Quality Palliative Care across Europe for Cancer and Dementia: International Challenges.

E N D
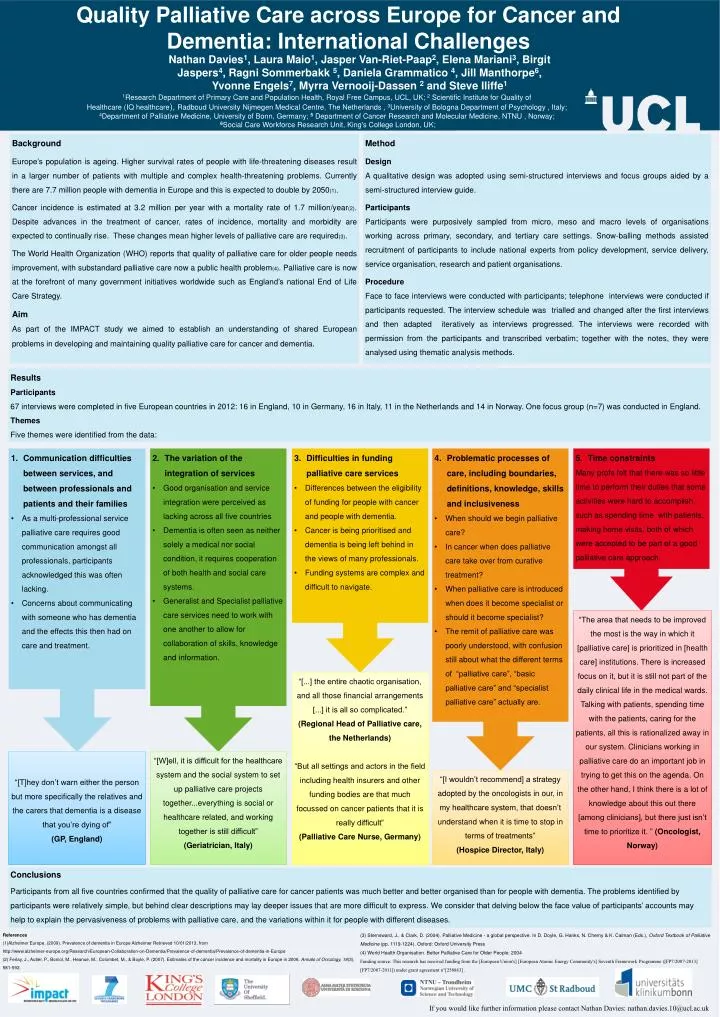
Quality Palliative Care across Europe for Cancer and Dementia: International Challenges Nathan Davies1, Laura Maio1, Jasper Van-Riet-Paap2, Elena Mariani3, Birgit Jaspers4, Ragni Sommerbakk 5, Daniela Grammatico 4, Jill Manthorpe6, Yvonne Engels7, Myrra Vernooij-Dassen 2 and Steve Iliffe1 1Research Department of Primary Care and Population Health, Royal Free Campus, UCL, UK; 2 Scientific Institute for Quality of Healthcare (IQ healthcare), Radboud University Nijmegen Medical Centre, The Netherlands , 3University of Bologna Department of Psychology , Italy; 4Department of Palliative Medicine, University of Bonn, Germany; 5 Department of Cancer Research and Molecular Medicine, NTNU , Norway;6Social Care Workforce Research Unit, King's College London, UK; Background Europe’s population is ageing. Higher survival rates of people with life-threatening diseases result in a larger number of patients with multiple and complex health-threatening problems. Currently there are 7.7 million people with dementia in Europe and this is expected to double by 2050(1). Cancer incidence is estimated at 3.2 million per year with a mortality rate of 1.7 million/year(2). Despite advances in the treatment of cancer, rates of incidence, mortality and morbidity are expected to continually rise. These changes mean higher levels of palliative care are required(3). The World Health Organization (WHO) reports that quality of palliative care for older people needs improvement, with substandard palliative care now a public health problem(4). Palliative care is now at the forefront of many government initiatives worldwide such as England’s national End of Life Care Strategy. Aim As part of the IMPACT study we aimed to establish an understanding of shared European problems in developing and maintaining quality palliative care for cancer and dementia. Method Design A qualitative design was adopted using semi-structured interviews and focus groups aided by a semi-structured interview guide. Participants Participants were purposively sampled from micro, meso and macro levels of organisations working across primary, secondary, and tertiary care settings. Snow-balling methods assisted recruitment of participants to include national experts from policy development, service delivery, service organisation, research and patient organisations. Procedure Face to face interviews were conducted with participants; telephone interviews were conducted if participants requested. The interview schedule was trialled and changed after the first interviews and then adapted iteratively as interviews progressed. The interviews were recorded with permission from the participants and transcribed verbatim; together with the notes, they were analysed using thematic analysis methods. Results Participants 67 interviews were completed in five European countries in 2012: 16 in England, 10 in Germany, 16 in Italy, 11 in the Netherlands and 14 in Norway. One focus group (n=7) was conducted in England. Themes Five themes were identified from the data: • Communication difficulties between services, and between professionals and patients and their families • As a multi-professional service palliative care requires good communication amongst all professionals, participants acknowledged this was often lacking. • Concerns about communicating with someone who has dementia and the effects this then had on care and treatment. • The variation of the integration of services • Good organisation and service integration were perceived as lacking across all five countries • Dementia is often seen as neither solely a medical nor social condition, it requires cooperation of both health and social care systems. • Generalist and Specialist palliative care services need to work with one another to allow for collaboration of skills, knowledge and information. • Difficulties in funding palliative care services • Differences between the eligibility of funding for people with cancer and people with dementia. • Cancer is being prioritised and dementia is being left behind in the views of many professionals. • Funding systems are complex and difficult to navigate. • Problematic processes of care, including boundaries, definitions, knowledge, skills and inclusiveness • When should we begin palliative care? • In cancer when does palliative care take over from curative treatment? • When palliative care is introduced when does it become specialist or should it become specialist? • The remit of palliative care was poorly understood, with confusion still about what the different terms of “palliative care”, “basic palliative care” and “specialist palliative care” actually are. • Time constraints • Many profs felt that there was so little time to perform their duties that some activities were hard to accomplish, such as spending time with patients, making home visits, both of which were accepted to be part of a good palliative care approach. “The area that needs to be improved the most is the way in which it [palliative care] is prioritized in [health care] institutions. There is increased focus on it, but it is still not part of the daily clinical life in the medical wards. Talking with patients, spending time with the patients, caring for the patients, all this is rationalized away in our system. Clinicians working in palliative care do an important job in trying to get this on the agenda. On the other hand, I think there is a lot of knowledge about this out there [among clinicians], but there just isn’t time to prioritize it. ” (Oncologist, Norway) “[...] the entire chaotic organisation, and all those financial arrangements [...] it is all so complicated.” (Regional Head of Palliative care, the Netherlands) “But all settings and actors in the field including health insurers and other funding bodies are that much focussed on cancer patients that it is really difficult” (Palliative Care Nurse, Germany) “[T]hey don’t warn either the person but more specifically the relatives and the carers that dementia is a disease that you’re dying of” (GP, England) “[W]ell, it is difficult for the healthcare system and the social system to set up palliative care projects together...everything is social or healthcare related, and working together is still difficult” (Geriatrician, Italy) “[I wouldn’t recommend] a strategy adopted by the oncologists in our, in my healthcare system, that doesn’t understand when it is time to stop in terms of treatments” (Hospice Director, Italy) Conclusions Participants from all five countries confirmed that the quality of palliative care for cancer patients was much better and better organised than for people with dementia. The problems identified by participants were relatively simple, but behind clear descriptions may lay deeper issues that are more difficult to express. We consider that delving below the face value of participants’ accounts may help to explain the pervasiveness of problems with palliative care, and the variations within it for people with different diseases. References (1)Alzheimer Europe. (2009). Prevalence of dementia in Europe Alzheimer Retrieved 10/01/2013, from http://www.alzheimer-europe.org/Research/European-Collaboration-on-Dementia/Prevalence-of-dementia/Prevalence-of-dementia-in-Europe (2) Ferlay, J., Autier, P., Boniol, M., Heanue, M., Colombet, M., & Boyle, P. (2007). Estimates of the cancer incidence and mortality in Europe in 2006. Annals of Oncology, 18(3), 581-592. (3) Sternsward, J., & Clark, D. (2004). Palliative Medicine - a global perspective. In D. Doyle, G. Hanks, N. Cherny & K. Calman (Eds.), Oxford Textbook of Palliative Medicine (pp. 1119-1224). Oxford: Oxford University Press (4) World Health Organisation. Better Palliative Care for Older People. 2004 Funding source: This research has received funding from the [European Union's] [European Atomic Energy Community's] Seventh Framework Programme ([FP7/2007-2013] [FP7/2007-2011]) under grantagreement n°[258883] . If you would like further information please contact Nathan Davies: nathan.davies.10@ucl.ac.uk