Download
1 / 1
10 likes | 158 Views
Pediatric Transfers From a Community ED: Does Care or Diagnosis Change? N. Molinaro , DO, A. Mehta , DO, B. Abo , DO, F. Azubuike , MD. Introduction. Methods. Discussion. Results.

E N D
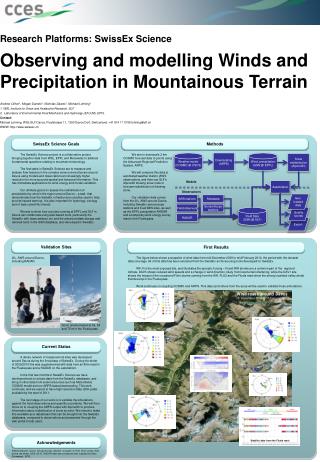
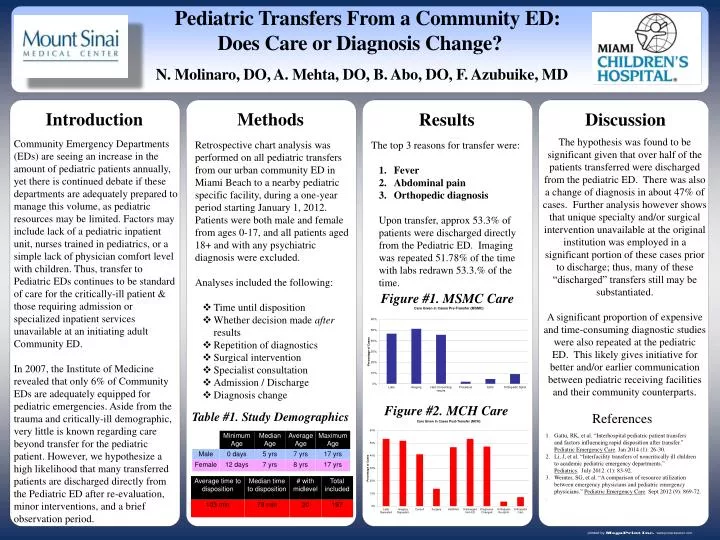
Pediatric Transfers From a Community ED: Does Care or Diagnosis Change? N. Molinaro, DO,A. Mehta, DO,B. Abo, DO, F. Azubuike, MD Introduction Methods Discussion Results The hypothesis was found to be significant given that over half of the patients transferred were discharged from the pediatric ED. There was also a change of diagnosis in about 47% of cases. Further analysis however shows that unique specialty and/or surgical intervention unavailable at the original institution was employed in a significant portion of these cases prior to discharge; thus, many of these “discharged” transfers still may be substantiated. A significant proportion of expensive and time-consuming diagnostic studies were also repeated at the pediatric ED. This likely gives initiative for better and/or earlier communication between pediatric receiving facilities and their community counterparts. • Retrospective chart analysis was performed on all pediatric transfers from our urban community ED in Miami Beach to a nearby pediatric-specific facility, during a one-year period starting January 1, 2012. Patients were both male and female from ages 0-17, and all patients aged 18+ and with any psychiatric diagnosis were excluded. Analyses included: • Overall time of transfer • Decision made after concerning result • Repetition of diagnostics • Surgical intervention • Specialist consultation • Admission / Discharge • Diagnosis change Community Emergency Departments are seeing an increase in the amount of pediatric patients annually, yet there is continued debate if these departments are adequately prepared to manage the pediatric patient, as pediatric resources may be limited. Transfer to Pediatric EDs continues to be standard of care for the critically-ill patient and those requiring admission or specialized inpatient services unavailable at an initiating Community ED. However, we hypothesize that it is likely that many transferred patients are discharged directly from the Pediatric ED after re-evaluation, minor interventions, and a brief observation period. Community Emergency Departments (EDs) are seeing an increase in the amount of pediatric patients annually, yet there is continued debate if these departments are adequately prepared to manage this volume, as pediatric resources may be limited. Factors may include lack of a pediatric inpatient unit, nurses trained in pediatrics, or a simple lack of physician comfort level with children. Thus, transfer to Pediatric EDs continues to be standard of care for the critically-ill patient & those requiring admission or specialized inpatient services unavailable at an initiating adult Community ED. In 2007, the Institute of Medicine revealed that only 6% of Community EDs are adequately equipped for pediatric emergencies. Aside from the trauma and critically-ill demographic, very little is known regarding care beyond transfer for the pediatric patient. However, we hypothesize a high likelihood that many transferred patients are discharged directly from the Pediatric ED after re-evaluation, minor interventions, and a brief observation period. • Retrospective chart analysis was performed on all pediatric transfers from our urban community ED in Miami Beach to a nearby pediatric specific facility, during a one-year period starting January 1, 2012. Patients were both male and female from ages 0-17, and all patients aged 18+ and with any psychiatric diagnosis were excluded. • Analyses included the following: • Time until disposition • Whether decision made after results • Repetition of diagnostics • Surgical intervention • Specialist consultation • Admission / Discharge • Diagnosis change • The top 3 reasons for transfer were: • Fever • Abdominal pain • Orthopedic diagnosis • Upon transfer, approx 53.3% of patients were discharged directly from the Pediatric ED. Imaging was repeated 51.78% of the time with labs redrawn 53.3.%of the time. Figure #1. MSMC Care Figure #2. MCH Care Table #1. Study Demographics References Gattu, RK, et al. “Interhospital pediatric patient transfers and factors influencing rapid disposition after transfer.” Pediatric Emergency Care. Jan 2014 (1): 26-30. Li, J, et al. “Interfacility transfers of noncritically ill children to academic pediatric emergency departments.” Pediatrics. July 2012. (1): 83-92. Weinter, SG, et al. “A comparison of resource utilization between emergency physicians and pediatric emergency physicians.” Pediatric Emergency Care. Sept 2012 (9): 869-72. .