Download
1 / 30
300 likes | 466 Views
Results of Sentinel Sites Study. Dr Karin Denton. HPV testing as a triage for women with low grade cytological abnormalities: results from the sentinel sites studies. Kelly R, Patnick J, Kitchener HC, Moss SM Br J Cancer. 2011 Sep 27;105(7):983-8. Results.

E N D
Results of Sentinel Sites Study Dr Karin Denton
HPV testing as a triage for women with low grade cytological abnormalities: results from the sentinel sites studies. Kelly R, Patnick J, Kitchener HC, Moss SM Br J Cancer. 2011 Sep 27;105(7):983-8.
Results Study took place between 1 Jan 2008 and 1 April 2009 Data collected until September 2009 Analysis conducted independently at Cancer Screening Evaluation Unit, Institute of Cancer Research Over 90% of women attended colposcopy North Bristol NHS Trust/Avon Cervical screening programme
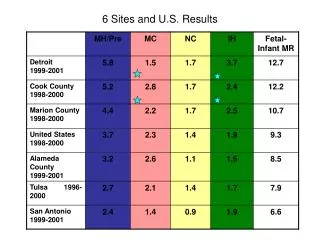
HPV positive rates by age group and initial cytology result North Bristol NHS Trust/Avon Cervical screening programme
SSS Results from different centresHPV positive rate by site and initial cytology 1 North Bristol NHS Trust/Avon Cervical screening programme
SSS Results from different centresHPV positive rate by site and initial cytology 2 North Bristol NHS Trust/Avon Cervical screening programme
Sentinel Site StudyResults at colposcopy *Includes 3 invasive cancers North Bristol NHS Trust/Avon Cervical screening programme
Sentinel Site StudyPPV of colposcopy by site 1 North Bristol NHS Trust/Avon Cervical screening programme
Sentinel Sites StudyRate of disease at 1, 2 3 and >3 years after negative colposcopy in 956 women with long term follow-up North Bristol NHS Trust/Avon Cervical screening programme
Test of Cure • Preliminary data only in un-triaged women • 3203 women had test of cure • Failed test of cure by 18.3% • 6.2% by abnormal cytology • 12.1% by HPV +ve with normal cytology • Increased ‘failure’ rates with lower CIN grade • Persistent CIN2+ in 7% • 3% in HPV +ve • 13% in cytology +ve North Bristol NHS Trust/Avon Cervical screening programme
Bristol Outcome Lletz histology for mild and borderline HPV positive smears with CIN 2/3 on PB(%)
National outcomes • 90% attendance • Half had PB (47% negative histology) • 2.4% had LLETZ ( 28% neg histology) • 1/3 of identified CIN1 were not treated • Apparent overall cytological progression was 3.4% at 12 months
Management outcome in women referred to Colposcopy following HPV Test of Cure (TOC) Mohini Vachhani, Mary Brett*, Anne Vaughton, Vikki Finch, John Murdoch Colposopy Clinic and *Cellular Pathology Dept, Southmead Hospital Presented 22/06/2011 (Also, poster at BSCCP meeting 31.3-1.4/2011)
Results • No of samples with HPV TOC test = 2369 • HPV negative = 2017 (85%) routine recall • HPV positive = 352 (15% - National rate18%) colposcopy • Referred to Southmead = 141 • Referred to St Michael’s = 211
Outcome • TZ seen; NAD –> Cytology follow up in Community (n = 66) • TZ seen; abnormality seen (n = 22): 2 LLETZ (CIN 1, CIN2) 16 biopsy (3 CIN1, 13 neg) 4 rpt cytology (all negative)
Outcome • Colposcopy was unsatisfactory in 30% of cases (i.e.TZ not seen): n = 38 • 6 had further LLETZ (all negative) • 13 had Bx (1 CIN 1, 12 neg)
Outcome • Total no with repeat LLETZ = 8 cases • 7 had involved margins in index LLETZ • 2/8 with satisfactory colp and abnormality seen (Histo: CIN1, CIN2) • 6/8 with unsatisfactory colp (Histo: all negative)
Conclusion • Women with positive TOC are at minimal risk of residual CIN (6/126 =4.8%) • 5/126 (4%) = CIN1 • 1/126 (0.8%) = CIN2 • Nationally PPV for CIN2 or worse = 2.9% and for CIN3 or worse = 0.4%
Other studies H Kitchener et al. BJOG 2008, 15(8): 1001-1007 • Of cyto neg/HPV pos referrals to colp, 9/75 had CIN (at 6, 12 or 24 months follow up post-LLETZ; 4 CIN1, 4 CIN2, 1 CIN3) • = 12% treatment failure rate. (Compared with Southmead data: 6/126 had residual CIN = 4.8%)
Changes to KC61? Don’t panic, no change to data collection or categories
Longer term impact on KC61 data • BC rate will fall (due to loss of 2nd and 3rd bc) • Mild rate will also fall depending on previous policy • Will be visible effect from year 1 • High grade rate will also fall slightly because women will be referred on a prior low grade result
Caution • You must decide on a diagnosis and stick to it regardless of HPV result • Do not use BC?HG in order to get an HPV test • Follow the management protocol
ABC3 • ? Launch date • Will abolish BC?HG
KEY TO CODES & ABBREVIATIONS Action codes • A routine recall • Rm early repeat in 'm' months • S suspend from recall PROVISIONAL Result codes • Ø * ?glandular neoplasia (non cervical) • G * ?glandular neoplasia (non cervical) (HPV tested) • 1 inadequate • 2 negative (not HPV tested) • N negative (HPV tested) • 3 low grade dyskaryosis (not HPV tested) • M low grade dyskaryosis (HPV tested) • 4 high grade dyskaryosis (severe) • 5 high grade dyskaryosis ?invasive squamous carcinoma • 6 ?glandular neoplasia of endocervical type • 7 high grade dyskaryosis (moderate) • 8 borderline change in squamous cells (not HPV tested) • B borderline change in squamous cells (HPV tested) • 9 borderline change in endocervical cells • E borderline change in endocervical cells (HPV tested)
* non-cervical neoplasia treated as negative for CSP management • Infection codes • Ø (zero) HPV negative • 9 (nine) HPV positive • U HPV result inadequate/unreliable • Miscellaneous • NTDD Next Test Due Date • BLUE indicates codes used on NHAIS in format • Cytology result – HPV infection code – Action code • RED indicates manual action required to reset NTDD