Download
1 / 15
180 likes | 444 Views
Anticoagulant Drug Information. Anticoagulants are prescribed to patients who are at an increased risk for developing blood clots. Anticoagulants reduce blood clotting in several ways.

E N D
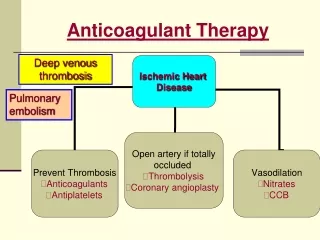
Anticoagulant Drug Information • Anticoagulants are prescribed to patients who are at an increased risk for developing blood clots. • Anticoagulants reduce blood clotting in several ways. - This prevents complications of blood clots such as deep vein thrombosis, pulmonary embolism, myocardial infarction and stroke - Also used after major orthopedic surgeries.
Drug Information • Warfarin – Vitamin K antagonist - Inhibits several coagulation factors (I, V, VII, etc.) - Most effective in strictly regulated INR ratio of 2.0-3.0 - Must be monitored and adjusted by monthly blood draws to ensure INR between 2-3 • Dabigatran (Dabi, Pradaxa™) - Direct Thrombin Inhibitor - Does not require monitoring - Effects cannot be reversed (unlike Warfarin)
Dabigatranvs warfarin in patients with Atrial Fibrillation: RE-LY trial • Noninferiority trial • 18,133 patients with atrial fibrillation at risk for stroke (951 clinical centers, 44 countries) • 3 Treatment groups: • Dabigatran: BLINDED • 110 mg or 150 mg capsules twice daily • Warfarin: UNBLINDED • Tablets of 1, 3, or 5 mg daily; adjusted to INR of 2-3 (measured at least monthly) • Median follow up of 2 years, same follow up visit schedule for the 3 groups • 99.9% of patients achieved complete follow-up NEJM 2009;361:1139-51
Dabigatranvs warfarin in patients with Atrial Fibrillation: RE-LY trial • Primary study outcome: stroke or systemic embolism • Primary safety outcome: major hemorrhage • Each outcome adjudicated by 2 independent reviewers unaware of treatment allocation NEJM 2009;361:1139-51
Dabigatranvs warfarin in patients with Atrial Fibrillation: RE-LY trial • Results: • Both doses of dabigatranwere non-inferior to warfarin • Dabigatran 150 mg superior to warfarin in preventing primary outcome • Compared to warfarin, fewer rates of hemorrhagic stroke in Dabigatran 110 mg and 150 mg • Compared to warfarin, fewer rates of major bleeding in Dabigatran 110 mg but not 150 mg • More GI bleeding with Dabigatran 150 mg than warfarin ( • Higher rates of discontinuation with dabi (21 vs 17%) • Dyspepsia only AE significantly more common in dabigatranvs warfarin NEJM 2009;361:1139-51
Lancet article: further analysis of RE-LY trial • Mean INR time in the therapeutic range (TTR) for warfarin patients in NEJM trial was 64% • Lancet article evaluated primary and secondary outcomes in relation to each center's mean TTR in the warfarin group • 4 quartiles: <57.1%, 51.7-65.5%, 65.5 – 72.6%, >72.6% • Findings similar regardless of quartile- results “consistent irrespective on centers' quality of INR control” Lancet 2010;376:975-83
Discussion Question • The FDA strongly encourages blinded trials for pivotal studies. • Was it reasonable to conduct an open label comparison of dabigatran with warfarin?
Blinding • Definition: Patients and/or investigators are prevented from knowing certain information during the trial that might lead to bias 1. treatment assigned 2. endpoint assessment • Goal: To eliminate bias associated with physician/patient being aware of treatment that is rendered • To assure that all patients in all treatment groups are treated and evaluated in a similar way • Different from bias prevented with randomization
Would blinding be feasible or reasonable in RE-LY? • We considered • Ethics (undue harm to patient) • Practicality (similarity of treatments) • Bias (potential and observed) • Compromise (partial blinding)
Would blinding be ethical in RE-LY? • Blinding would necessitate unnecessary monthly blood draws in the dabigatran arm • Life threatening bleeding • Time to “break the blind” may be too long • There are various methods of warfarin reversal that can work rapidly (minutes) or over days, and labs indicate the level of anticoagulation • There is no antidote to dabigatran (supportive care, attempts to remove drug from blood) and labs do not indicate the level of anticoagulation
Would blinding to treatment be practical in RE-LY? • The treatments differ in important ways • Formulation: tablets vs capsules • Dose schedule: daily (warfarin) vs. BID (dabi) • Monitoring: monthly blood draws vs. none • Dose adjustment: warfarin adjusted based on INR, and coordinating center was instructing the local centers how to best adjust the dose • Diet and medication interactions • They did blind to treatment when it was practical • Dose of dabi (110 vs 150)
Potential for bias in RE-LY • A systematic error in the design or conduct of a study that leads to incorrect estimates of treatment effect • Information bias • Participant Bias: unblinded subjects exaggerate the effects or are more likely to report benefit or AE of study med • Non-issue with primary outcomes (stroke, embolism) • Maybe for subjective outcome: Dyspepsia (Dabi group) • Observer Bias: knowledge of treatment arm by the outcome assessor may cause differential ascertainment & diagnosis of endpoints • Outcome events were adjudicated by 2 independent investigators blinded to treatment assignments.
Potential for bias in RE-LY • Differential ancillary/compensatory treatment • Similar monitoring schedule but warfarin patients may receive more care/counseling after monthly blood draws • Knowledge of treatment may have affected decision to stay on study drug • Could not objectively assess adherence to dabi • Rates of discontinuation at 1 and 2 years were higher with dabigatran than with warfarin
Did the design affect the analysis? • Researchers appeared to use similar intention to treat analysis as to those for blinded trials • Investigated and tested relationships between variables to determine if the lack of blinding led to the observed outcome • Tests showed that lack of blinding did not appear to skew the results to favor any one treatment • “The unexpectedly different rates of myocardial infarction and gastrointestinal bleeding among the three treatment groups support an absence of bias.” NEJM 2009;361:1139-51
Compromise (partial blinding) • Dabi arm double blind to dose • Endpoint assessment was blinded CONCLUSION: As conducted with open label treatment and blinded endpoint assessment, the study followed the most ethical, practical and reasonable design and did not introduce significant bias.