Download
1 / 78
990 likes | 2.06k Views
INTRODUCTION to LOCAL ANESTHESIA and NEUROPHYSIOLOGY. Definition of Local Anesthesia. a loss of sensation in a circumscribed area of the body caused by a depression of excitation in nerve endings Or

E N D
Definition of Local Anesthesia a loss of sensation in a circumscribed area of the body caused by a depression of excitation in nerve endings Or an inhibition of the conduction process in peripheral nerves; no loss of consciousness occurs
Properties of Local Anesthetics: 1) Not irritating to the tissue 2) No permanent alteration of nerve structure 3) Systemic toxicity should be low 4) Effective whether injected or applied topically 5) Time of onset of anesthesia should be as short as possible 6) Duration of action must be long enough to complete the procedure but not so long as to require an extended recovery 7) Should be stable in solution and easily biotransformed 8) Should not cause allergic reactions 9) Should be sterile or capable of being sterilized by use of heat
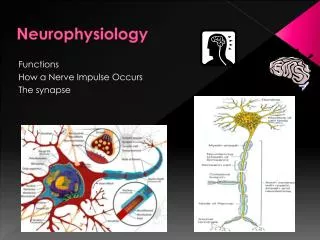
Neurophysiology • The Neuron • The neuron is the structural unit of the nerve • Two types of neurons • 1) Sensory afferent (toward the CNS) • 2) Motor efferent (away from the CNS)
Sensory Neurons: transmit pain; three parts1) Dendritic Zone- free nerve endings; most distal portion of the neuron2) Axon- synapses with the CNS to transmit input to the brain3) Cell Body- provides metabolic support for the entire neuron
The Axon • long cylinder of neural cytoplasm (axoplasm) encased in a • thin sheath, the nerve membrane, or axolemma • axoplasm is a gelatinous substance that is separated from • extracellular fluids by a continuous nerve membrane
nerve cell membrane is ~75 Angstroms thick • all cell membranes are organized to block the diffusion of water • soluble molecules • all cell membranes are selectively permeable via specialized pores • transduce information by protein receptors responsive to chemical or • physical stimulation by neurotransmitters, hormones, light, vibrations
The Membrane • cell membrane is a bilipidlayer of phospholipids • hydrophilic (polar) ends facing the outer surface and • hydrophobic (nonpolar) ends projecting to the middle of • the membrane
the nerve membrane lies at the interface between the extracellular fluid and the axoplasmthe nerve membrane separates highly ionic concentrations within the axon from those outside
The Membranethe resting nerve membrane has an electrical resistance about 50 times greater than that of the extra/intracellular fluids, thus preventing the passage of Na, K and Cl ions down their concentration gradientswhen a nerve impulse passes, electrical conductivity of the nerve membrane increases 100-fold: increased conductivity allows the passage of Na and K ions down their concentration gradient through the nerve membranemovement of these ions provides the energy for impulse conduction along the nervesome nerve fibers are covered in myelin, specialized Schwann cells
regular interval constrictions are called Nodes of Ranvier which form gaps between two adjoining Schwann cells
Electrophysiology of Nerve Conduction • Nerve resting potential is-70 mV; this is produced by differing concentrations of ions • on either side of the nerve membrane • Interior of the nerve is negative compared to the exterior before a stimulus excites the nerve
STEP 1 - Stimulus excites nerve which leads to:1) Slow Depolarization- inside of nerve becomes less negative2) Threshold Potential- extremely rapid depolarization occurs from the falling electrical potential3) Rapid Depolarization- interior is electrically positive +40 mV and the outside is negative(-70 mv)
STEP 2 - after depolarization, repolarization occursRepolarization- electric potential inside the cell gradually becomes more negative until the interior is again restored to –70 mV
Depolarization-excitation leads to increase in permeability of the cell membrane to sodium ions-transient widening of transmembrane ion channels allow passage of the sodium ions-rapid influx of sodium ions into the interior of the nerve cell causes depolarization of the cell membrane from resting to firing threshold which is -50 to -60 mV
Firing Threshold magnitude of the decrease in negative trans-membrane potential that is necessary to initiate an action potential (impulse); getting more positive with more influx of Na+
-decrease in negative transmembrane potential of +15 mV; from –70 mV to –55 mV is necessary to reach the firing threshold; voltage differences of less than +15 mV will not induce firing-exposure to a nerve with local anesthetic raises its firing threshold-elevating the firing threshold means that more sodium must pass through the membrane to decrease the negative transmembrane potential to a level where depolarization occurs
-when the firing threshold is reached, sodium rapidly enters the axoplasm due to increased membrane permeability-depolarization lasts ~ .3 msec
RepolarizationThe action potential is terminated when the membrane repolarizes; this is caused by the inactivation of increased permeability to sodiumThe movement of Na+ and K+ during depolarization is passive
After the membrane potential returns to –70 mV there is still a slight amount of excess sodium within the nerve cell and a slight excess of potassium extracellularlySodium is moved out of the cell using ATP and the sodium pumpRepolarization requires ~ .7 msec
Absolute Refractory Period the nerve is unable to respond to another stimulus regardless of its strengthRelative Refractory Period a new impulse can be initiated at this time but only by a stronger than normal stimulus; follows the absolute refractory period
Membrane ChannelsSodium channels line the excitable nerve membrane which are lipoglycoproteins situated firmly in the membranesSodium passes through the channels 12 times easier than potassiumSodium ions are “thinner” than potassium or chloride ions and should therefore move easily down concentration gradients through membrane channels into the nerve cell, however:However, sodium ions are hydrated at rest and increase in size to 3.4 Angstroms; they are too large to pass through the sodium channels when the nerve is at rest
Membrane ChannelsPotassium and chloride can pass through these gated channelsDuring depolarization the gated transmembrane sodium channels change their configuration to allow the sodium ions to enter the cell
Impulse PropagationActivation of an action potential by a stimulusDisruption of the resting nerve membrane potentialInterior of the cell goes from negative (–70 mV) to positive (+40 mV)Exterior of the cell changes from positiveto negativeLocal currents begin flowing between the depolarized segment and the adjacent resting areaLocal currents flow from positive to negative extending for several mm along the nerve membraneAs a result, the interior of adjacent areas become less negative and the exterior becomes less positive
Impulse PropagationTransmembrane potential decreases approaching firingthreshold for depolarizationWhen transmembrane potential decreases by 15mV from resting potential, firing threshold is reached and rapid depolarization occursThe newly depolarized segment sets up local currents and it all starts over againNewly depolarized segments return to resting state after absolute and relative refractory periodsWaves of depolarization can move in only one direction due to the absolute and relative refractory periods, thus retrograde (backward) movement is prevented
Impulse Spread 1) Unmyelinated Nerves -high electrical resistance cell membrane -slow forward “creeping” spread of impulses -conduction of unmyelinated C fibers is1.2 m/sec
2) Myelinated Nerves -insulating myelin separates the extra/intracellular charges -the farther apart the charges the smaller the current necessary to charge the membrane -current leaps from node to node saltatory conduction
Myelinated Nerves if conduction of an impulse is blocked at one node, the local current skips that node and continues to the next node
A minimum of 8 to 10 mm of nerve mustbe covered by anesthetic solution to ensure adequate block of impulse spread
Mode and Site of Action of Local Anesthetics Local anesthetics interfere with the excitation process in the nerve membrane in one or more of the following ways: 1) Altering the basic resting potential of the nerve membrane 2) Altering the threshold potential (firing level) 3) Decreasing the rate of depolarization* 4) Prolonging the rate of repolarization
Because of local anesthetics, cellular depolarization is not sufficient to reduce the membrane potential of a nerve fiber to its firing threshold and a propagated action potential does not develop
Where Do Local Anesthetics Work? Specific Receptor Theory local anesthetics act by binding to specific receptors on the sodium channel the action of the drug is direct and is not mediated by some change in the general properties of the cell membrane a specific receptor site for local anesthetics exists in the sodium channel which eliminates permeability to sodium ions Therefore: no impulse conduction
Tertiary amine local anesthetics inhibit influx of sodium during nerve conduction
Mechanism of Action of Local Anesthetics 1) Displacement of calciumions from the sodium channel receptor site 2) Binding of the local anesthetic molecule to this receptor site 3) Blockade of the sodium channel 4) Decrease in sodium conductance 5) Depression of the rate of electrical depolarization 6) Failure to achieve the threshold potential level (firing level) 7) Lack of development of propagated action potentials 8) Conduction blockade
1) The nerve remains in a polarized state, therefore there is no depolarization because the ionic movements responsible for the action potential fail to develop2) The membrane’s electrical potential remains unchanged, therefore local currents do notdevelop and the self-perpetuating mechanism of impulse propagation is stalled3) Nerve block produced by local anesthetic is called a nondepolarizing nerve block
Local Anesthetic Molecules Majority of local anesthetics are tertiaryamines (except Prilocaine) All local anesthetics are amphipathic (lipophilic/hydrophilic)
Three main parts of the local anesthetic molecule:1) Lipophilic Part (aromatic ring)2) Intermediate Chain (amide or ester)3) Hydrophilic Part (ethyl alcohol/acetic)
The lipophilicpart of the local anesthetic is the largest portion of the molecule Hydrophilic part of the local anesthetic is an amino derivative of ethyl alcohol or acetic acid Local anesthetics without a hydrophilic portion are not suitable for injection but are good topical anesthetics, i.e., Benzocaine
What Form Do Local Anesthetics Exist in the Cartridge? Labs prepare local anesthetics as basic: poorly soluble in water and unstable on exposure to air; they have little to no clinical value in this state Since they are weakly basic, they combine readily with acids to form local anesthetic salts which makes them soluble in water and stable