Download
1 / 1
30 likes | 499 Views
The Use of Neurofeedback in Military Post-traumatic Stress Disorder. Pearson, Heather J, BSc, MD, FRCPC*, McCulloch, Janet, MD, CCFP, FRCPC, Beckett, Linda, MD, CCFP*. *Department of Psychiatry, Queen’s University, Kingston, Ontario, Canada. OPTIONAL LOGO HERE. Background. About this template.

E N D
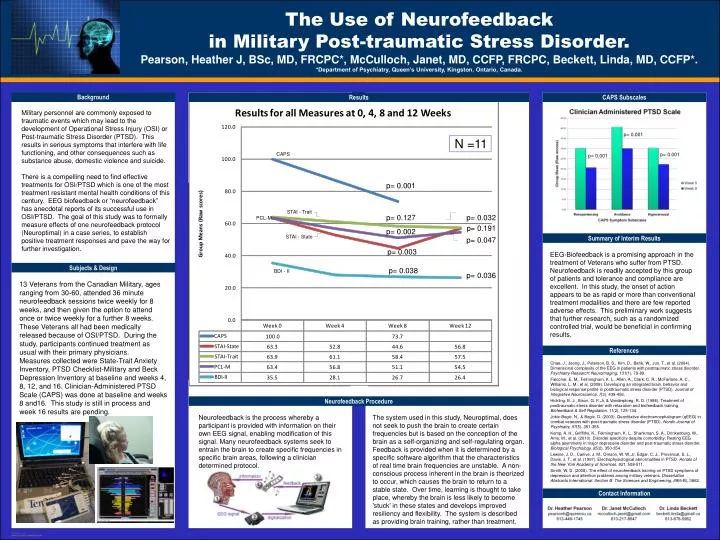
The Use of Neurofeedback in Military Post-traumatic Stress Disorder. Pearson, Heather J, BSc, MD, FRCPC*, McCulloch, Janet, MD, CCFP, FRCPC, Beckett, Linda, MD, CCFP*.*Department of Psychiatry, Queen’s University, Kingston, Ontario, Canada. OPTIONALLOGO HERE Background About this template Results CAPS Subscales Military personnel are commonly exposed to traumatic events which may lead to the development of Operational Stress Injury (OSI) or Post-traumatic Stress Disorder (PTSD). This results in serious symptoms that interfere with life functioning, and other consequences such as substance abuse, domestic violence and suicide. There is a compelling need to find effective treatments for OSI/PTSD which is one of the most treatment resistant mental health conditions of this century. EEG biofeedback or “neurofeedback” has anecdotal reports of its successful use in OSI/PTSD. The goal of this study was to formally measure effects of one neurofeedback protocol (Neuroptimal) in a case series, to establish positive treatment responses and pave the way for further investigation. p= 0.001 N =11 CAPS p= 0.001 p= 0.001 p= 0.001 STAI - Trait p= 0.127 p= 0.032 PCL-M p= 0.191 p= 0.002 STAI - State Summary of Interim Results p= 0.047 EEG-Biofeedback is a promising approach in the treatment of Veterans who suffer from PTSD. Neurofeedback is readily accepted by this group of patients and tolerance and compliance are excellent. In this study, the onset of action appears to be as rapid or more than conventional treatment modalities and there are few reported adverse effects. This preliminary work suggests that further research, such as a randomized controlled trial, would be beneficial in confirming results. p= 0.003 Subjects & Design p= 0.038 BDI - II p= 0.036 13 Veterans from the Canadian Military, ages ranging from 30-60, attended 36 minute neurofeedback sessions twice weekly for 8 weeks, and then given the option to attend once or twice weekly for a further 8 weeks. These Veterans all had been medically released because of OSI/PTSD. During the study, participants continued treatment as usual with their primary physicians. Measures collected were State-Trait Anxiety Inventory, PTSD Checklist-Military and Beck Depression Inventory at baseline and weeks 4, 8, 12, and 16. Clinician-Administered PTSD Scale (CAPS) was done at baseline and weeks 8 and16. This study is still in process and week 16 results are pending. References Chae, J., Jeong, J., Peterson, B. S., Kim, D., Bahk, W., Jun, T., et al. (2004). Dimensional complexity of the EEG in patients with posttraumatic stress disorder. Psychiatry Research: Neuroimaging, 131(1), 79-89. Falconer, E. M., Felmingham, K. L., Allen, A., Clark, C. R., McFarlane, A. C., Williams, L. M., et al. (2008). Developing an integrated brain, behavior and biological response profile in posttraumatic stress disorder (PTSD). Journal of Integrative Neuroscience, 7(3), 439-456. Hickling, E. J., Sison, G. F.,Jr, & Vanderploeg, R. D. (1986). Treatment of posttraumatic stress disorder with relaxation and biofeedback training. Biofeedback & Self Regulation, 11(2), 125-134. Jokic-Begic, N., & Begic, D. (2003). Quantitative electroencephalogram (qEEG) in combat veterans with post-traumatic stress disorder (PTSD). Nordic Journal of Psychiatry, 57(5), 351-355. Kemp, A. H., Griffiths, K., Felmingham, K. L., Shankman, S. A., Drinkenburg, W., Arns, M., et al. (2010). Disorder specificity despite comorbidity: Resting EEG alpha asymmetry in major depressive disorder and post-traumatic stress disorder. Biological Psychology, 85(2), 350-354. Lewine, J. D., Canive, J. M., Orrison, W. W.,Jr, Edgar, C. J., Provencal, S. L., Davis, J. T., et al. (1997). Electrophysiological abnormalities in PTSD. Annals of the New York Academy of Sciences, 821, 508-511. Smith, W. D. (2008). The effect of neurofeedback training on PTSD symptoms of depression and attention problems among military veterans. Dissertation Abstracts International: Section B: The Sciences and Engineering, 69(6-B), 3862. Neurofeedback Procedure Neurofeedback is the process whereby a participant is provided with information on their own EEG signal, enabling modification of this signal. Many neurofeedback systems seek to entrain the brain to create specific frequencies in specific brain areas, following a clinician determined protocol. The system used in this study, Neuroptimal, does not seek to push the brain to create certain frequencies but is based on the conception of the brain as a self-organizing and self-regulating organ. Feedback is provided when it is determined by a specific software algorithm that the characteristics of real time brain frequencies are unstable. A non-conscious process inherent in the brain is theorized to occur, which causes the brain to return to a stable state. Over time, learning is thought to take place, whereby the brain is less likely to become 'stuck' in these states and develops improved resiliency and flexibility. The system is described as providing brain training, rather than treatment. Contact Information