Download
1 / 48
490 likes | 731 Views
Thyroid Physiology and NonThyroidal Illness. Gita Majdi March 2014. Outline. Thyroid hormone synthesis Action of thyroid hormone Nonthyroidal Illness . Thyroid. 35-30 grams in adults. Thyroid Follicle. Thyroid gland consists of numerous spherical follicles .

E N D
Thyroid Physiology and NonThyroidalIllness Gita Majdi March 2014
Outline • Thyroid hormone synthesis • Action of thyroid hormone • Nonthyroidal Illness
Thyroid 35-30 grams in adults
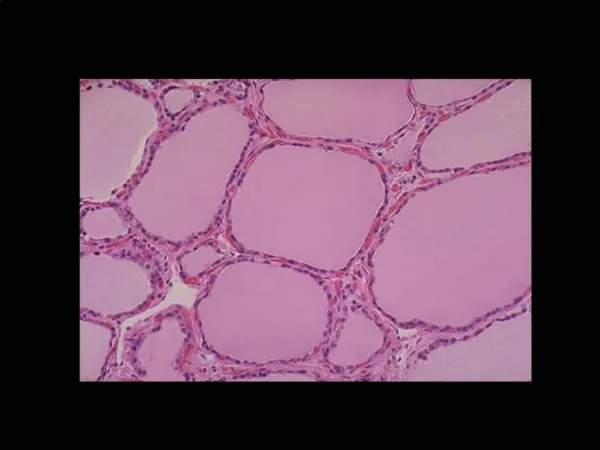
Thyroid Follicle Thyroid gland consists of numerous spherical follicles . Interior of the follicle is filled with the clear, proteinaceous material colloid, containing large amounts of thyroglobulin.
T4 Daily synthesis of 110 nmol/lit (85 mcg) of T4
From the apex of follicular cells, numerous microvilli extend into the follicle. Apical membrane : iodination, exocytosis and initial phase of hormone secretion occur Specific tyrosine residues of TG homodimers are iodinated at the apical borders of thyroid cells to form MIT & DIT. T4 &T3 are transported out of the phagolysosomes and across the basolateral cell membrane, exit the cell, and enter circulation.
Thyroid Hormone synthesis • Formation of normal quantities of thyroid hormone requires the availability of exogenous iodine. • At least 100 microgram of Iodine per day is required to eliminate all signs of iodine deficiency. • In healthy adult, absorption of iodide(I- ) is 90%. • Plasma iodide is completely filterable.(60-70% of filtered Ioad reabsorbed ). • The concentration of iodide in the extracelluar fluid is 10-15 mcg/lit. • Thyroid contains 8000 mcg of iodine.
Clinical Pearls Antithyroid drugs : Methimazole, Carbimazole and PTU inhibit TPO,sointrathyroidal iodine deficiency will happen.
TSH Receptor TSH Receptor has seven transmembrane domain , a large extracellular domain and a small intracellular domain. After activation receptor cleaves into α and β subunits. The α subunits is shed from the cell surface. The α subunit has TSH binding activity and it is water soluble.
Thyroid hormones in Peripheral tissue T4 concentration is highest and only arises from thyroid. 80% of T3 is derived from the peripheral tissues by enzymatic removal of a single 5’iodine atom from T4. The Plasma proteins with which T4 is mainly associated are TBG , transthyretin(TTR, formerly T4 binding pre albumin and albumin.
TBG Thyroxine Binding Globulin is a glycoprotein . There is one iodothyronine binding site per TBG molecule. TBG concentration is 270 nmol/lit ( 1.5 mcg/dl) The half life of protein in plasma is 5 days. Estrogen and acute hepatitis will increase TBG. TBG binding site has an affinity for T3 that is 20 fold less than that for T4. Binding of T4&T3 by TBG is inhibited by phenytoin, salicylate and furosemide . Patients receiving these medications have low total hormones.
Parameter T3 T4 • Production rate (nmol/day) 50 110 • Fraction from thyroid 0.2 1 • Relative metabolic potency 1 0.3 • Serum concentration • Total (nmol/L) 1.8 100 • Free (pmol/L) 5 20 • Distribution volume (L) 40 10 • Fraction intracellular 0.64 0.15 • Half-life (days) 0.75 6.7
Thyroid hormones in peripheral Tissue Cellular uptake and efflux of thyroid hormone is mediated by transporter proteins. Thyroid hormone transporter for T3 ,T4, rT3 and T2 : MCT 8 & OATP (monocarboxylate transporter ) OATP= organic anion transporting polypeptide Mutation in MCT8 gene has shown to cause severe developmental neurologic phenotype
Thyroid hormone in peripheral Tissues. T4 D1 & D2 T3 The T3 produced by D2(close to the nucleus) is especially effective In entering the nucleus and binding to thyroid hormone receptor. D2 serves the special purpose of prviding nuclear T3 from intracellular T4. T4 by D3 converts to rT3. T3 by D3 converts to T2. D3 is thyroid hormone inactivating enzyme . Highest D3 activity reported in infantile hemangioma (consumptive Hypothyroidism) D1,D2 and D3 contain rare amino acid selenocysteine. Preferred substrate for D1 is rT3. D1 is inhibited by PTU.
Thyroid hormone acts by binding to a specific nuclear receptors(TR) which inturn binds to DNA as a heterodimer with retinoid X receptor (RXR)at specific elements called TREs.(thyroid hormone response elements) T3 has a 15 fold higher affinity for TR than T4. In humans there are two TR genes, TRα and TRβ. (chromosome 17 &3)
Thyroid Receptor The active proteins are TRα and TR β1, Tβ2 and TRβ3. There are tissue specific preferences in expressions of the various TR. in human families with resistance to thyroid hormone, a condition in which TRβ mutations markedly reduce the binding affinity of TRβ for T3 were identified.
Thyroid hormone action Thyroid hormones are critical determinants of brain and somatic development in infants and of metabolic activity in adults; they also affect the function of virtually every organ system. Thyroid hormones must be constantly available to perform these functions.
Thyroid hormone Action: There are two thyroid hormone nuclear receptors (TR), alpha and beta . T3 binds to these TRs, and the T3-TR complexes then bind to regulatory regions contained in the genes that are responsive to thyroid hormone. TRs without T3 bind to nuclear receptor co-repressors and then to regulatory regions of genes normally induced by T3, resulting in repression of gene expression
Thyroid hormone, in the form of triiodothyronine (T3), acts by modifying gene transcription in virtually all tissues to alter rates of protein synthesis and substrate turnover. T3 has different actions in different tissues. These differences are determined by variations in both local production of T3 and the tissue distribution and content of TR isoforms. The deiodinases that convert the prohormone T4 to the active hormone T3 and convert T3 to diiodothyronines are also expressed in a development- and tissue-specific pattern
Thyroid Hormone Action • Thyroid hormones stimulate diverse metabolic activities most tissues, leading to an increase in basal metabolic rate. • One consequence of this activity is to increase body heat production, which seems to result, at least in part, from increased oxygen consumption and rates of ATP hydrolysis. • Lipid metabolism: Increased thyroid hormone levels stimulate fat mobilization, leading to increased concentrations of fatty acids in plasma. • They also enhance oxidation of fatty acids in many tissues. • Finally, plasma concentrations of cholesterol and triglycerides are inversely correlated with thyroid hormone levels - one diagnostic indication of hypothyroidism is increased blood cholesterol concentration.
Clinical Pearls • The identification of development- and tissue-specific pathways of thyroid hormone action is being translated into novel therapies. • Hypercholesterolemicpatients not at LDL target levels while on statins were given eprotirome (KB2115), a TR-beta selective agonist. Treatment for 12 weeks resulted in reduced total and LDL-cholesterol in all patients and also reduced triglycerides in those individuals with elevated baseline triglyceride levels. • A cardio-selective thyroid hormone analog, DITPA, has had some utility in treatment of congestive heart failure, although a longer study resulted in significant toxicity, especially metabolic, and the trial was stopped.
Thyroid hormone Action: • Carbohydrate metabolism: Thyroid hormones stimulate almost all aspects of carbohydrate metabolism, including enhancement of insulin-dependent entry of glucose into cells and increased gluconeogenesis and glycogenolysis to generate free glucose. • Growth: Thyroid hormones are clearly necessary for normal growth in children and young animals, as evidenced by the growth-retardation observed in thyroid deficiency. • The growth-promoting effect of thyroid hormones is intimately intertwined with that of growth hormone, a clear indication that complex physiologic processes like growth depend upon multiple endocrine controls.
Thyroid Hormone Action: • Development:Normal levels of thyroid hormone are essential to the development of the fetal and neonatal brain. • Cardiovascular system: Thyroid hormones increases heart rate, cardiac contractility and cardiac output. They also promote vasodilation, which leads to enhanced blood flow to many organs. • Central nervous system: Both decreased and increased concentrations of thyroid hormones lead to alterations in mental state. Too little thyroid hormone, and the individual tends to feel mentally sluggish, while too much induces anxiety and nervousness. • Reproductive system: Normal reproductive behavior and physiology is dependent on having essentially normal levels of thyroid hormone. Hypothyroidism in particular is commonly associated with infertility.
Thyroid Function in NonThyroidal Illness • Assessment of thyroid function in patients with nonthyroidal illness is difficult, especially among those hospitalized in an intensive care unit. • Many of them have low T4 andT3 and their serum thyrotropin TSH concentration also may be low. • Previously, these patients were thought to be euthyroid, and the term euthyroid-sick syndrome was used to describe the laboratory abnormalities . • There is some evidence that these patients may have acquired transient central hypothyroidism . • Despite these abnormalities, treatment of these patients with thyroid hormone, while controversial, appears to be of little benefit, and may be harmful. • It is possible that the changes in thyroid function during severe illness are protective in that they prevent excessive tissue catabolism.
NonThyroial Illness • Thyroid function should not be assessed in seriously ill patients unless there is a strong suspicion of thyroid dysfunction. • When thyroid dysfunction is suspected in critically ill patients, measurement of serum TSH alone is inadequate for the evaluation of thyroid function.
Low T3 The majority of hospitalized patients have low serum T3 concentrations, as do some outpatients who are ill.
Unlike T4, which is produced solely within the thyroid, 80 percent of circulating T3 is produced by the peripheral 5'-deiodination of T4 to T3, a reaction catalyzed by 5'-monodeiodinases in organs such as the liver and kidney. 5'-monodeiodination decreases whenever caloric intake is low and in any nonthyroidal illness, even mild illness. Reverse T3 (rT3) is the product of 5-monodeiodination of T4 (type III T4-5-deiodinase). The clearance of reverse T3 to diiodothyronine (T2) is reduced in nonthyroidal illness because of inhibition of the 5'-monodeiodinase activity As a result, serum rT3 concentrations are high in patients with nonthyroidal illnesses , except in those with renal failure and some with AIDS
Mechanisms of inhibition of 5'-monodeiodination and therefore low serum T3 concentrations in patients with nonthyroidal illness: 1-High endogenous serum cortisol concentrations and exogenous glucocorticoid therapy 2- Circulating inhibitors of deiodinase activity, such as free (non-esterified) fatty acids 3-Treatment with drugs that inhibit 5'-monodeiodinase activity such as amiodarone and high doses of propranolol. 4-Cytokines (such as tumor necrosis factor, interferon-alfaand interleukin-6).
FT4 Small reductions in binding proteins should not alter serum free T4 index or direct free T4 values, and these values are usually normal in patients whose illness is not severe.
Low T4 From 15 to 20 percent of hospitalized patients and up to 50 percent of patients in intensive care units have low serum T4 concentrations (low T4 syndrome). The concentrations are low primarily because of reductions in the serum concentrations of one or more of the three thyroid hormone-binding proteins. thyroxine-binding globulin (TBG), transthyretin (TTR, or thyroxine-binding prealbumin [TBPA]), and albumin.
FT4 Despite the theoretical attraction of measuring the concentration of free or biologically active hormone, it remains uncertain whether current free T4 methodology is any improvement over an uncontentious measurement of total T4“.
Possible contributing factors for decreased T4 and free T4: inhibitors of T4 binding • Some data support the possibility that high serum free fatty acid concentrations inhibit T4 binding to serum proteins. • Serum free fatty acid, particularly oleic acid concentrations, may be high in critically ill patients and their effect on T4 binding may be increased because of hypoalbuminemia. • Albumin is the major carrier of free fatty acids in serum. However, this phenomenon may be an in vitro effect of fatty acids released during collection and transport of the serum sample.
Transient Central Hypothyroidism (1) • Patients with severe nonthyroidal illness may have acquired transient central hypothyroidism. This suggestion is supported by the following observations: • A prospective study evaluated changes in thyroid function in patients undergoing bone marrow transplantation: serum TSH concentrations fell coincident with declines in serum T4 concentrations. • A study of critically ill patients recovering from nonthyroidal illness demonstrated that a rise in serum TSH concentration (which transiently reached supranormal values in some patients) preceded normalization of serum T4 concentrations. • Patients with nonthyroidal illness, similar to those with central hypothyroidism from other causes, have a blunted nocturnal rise in serum TSH concentrations, but usually have a normal serum TSH response to thyrotropin-releasing hormone (TRH) .
Central Hypothyroidism (2) • Abnormalities in TSH glycosylation that may decrease TSH bioactivity have been found in patients with nonthyroidal illness , and also in patients with central hypothyroidism. • TRH mRNA in the paraventricular nucleus of the hypothalamus was reduced in patients who died with nonthyroidal illness in one report, and was correlated with premortem serum T3 and TSH concentrations . • TRH infusion in patients with critical illness raises serum TSH, T4, and T3 concentrations. • Infusion of interferon-alfa to eight normal men caused a fall in serum TSH and T3 concentrations as well as a rise in the serum concentrations of rT3 and interleukin-6, thus mimicking the thyroid metabolic changes of serious illness, except that there was no fall in the serum T4 concentration.
Serum TSH • SERUM TSH — Serum TSH assays that have a detection limit of 0.01 mU/L should be used in assessing thyroid function in critically ill patients. TSH results should be interpreted as follows: • Low but detectable — Almost all patients who have a subnormal but detectable serum TSH concentration (greater than 0.05 mU/L and less than 0.3 mU/L) will be euthyroid when reassessed after recovery from their illness. • Undetectable — In contrast, approximately 75 percent of patients with undetectable serum TSH concentrations (<0.01 mU/L) have hyperthyroidism.
High TSH • Some hospitalized patients have transient elevations in serum TSH concentrations (up to 20 mU/L) during recovery from nonthyroidal illness. • Few of these patients prove to have hypothyroidism when reevaluatedafter recovery from their illness. • Patients with serum TSH concentrations over 20 mU/L usually have permanent hypothyroidism.
Prognosis • The magnitude of the changes in thyroid function in patients with nonthyroidal illness varies with the severity of the illness . • The serum T4 value correlates with outcome. • Similar findings were reported in a randomized trial of early versus late parenteral nutrition in critically ill ICU patients : • The patients who tolerated the nutritional deficit for one week had lower TSH, T4, T3, and T3/rT3 ratios . Lower T3, but higher T4 was associated with a higher likelihood of early alive ICU discharge. • These data suggest that inactivation of T4 to T3 conversion during starvation and illness may be a beneficial adaptation, while very low T4 levels in more critically ill patients are associated with deleterious outcomes.
TREATMENT • Thyroid hormone replacement has not been shown to be effective for patients with critical illness and low T3 and/or T4, or for patients undergoing cardiopulmonary bypass. • In a randomized trial of burn patients with low free T4 index and free T3 index levels, T3 replacement had no effect on mortality or metabolic rate when compared with placebo. • In a second trial, administration of T4 to 23 critically ill patients with low serum T4 concentrations did not alter either mortality or outcome.
CABG • During and after cardiopulmonary bypass, there is a transient decrease in serum T3 concentrations. • While animal data and anecdotal clinical experience had suggested that T3 repletion might improve outcomes after cardiopulmonary bypass , clinical trials have not demonstrated such a benefit. • In a systematic review of 14 randomized trials evaluating the administration of T3 in euthyroid adult patients in the immediate postoperative period (13 cardiac surgery, one renal transplantation), intravenous (IV) T3 administration increased cardiac index . • Mortality was not affected by high-dose IV T3 and could not be assessed for low dose IV or oral T3. • In one of the trials included in the meta-analysis, 142 patients with coronary heart disease undergoing coronary artery bypass surgery (CABG) were randomly assigned to intravenous T3 therapy (0.8 mcg/kg bolus followed by an infusion of 0.113mcg/kg/hour for six hours) at the completion of surgery or placebo . Although the mean cardiac index was higher and systemic vascular resistance was lower in the T3 group compared with placebo, there were no differences in the incidence of arrhythmia, need for inotropic or vasodilator drugs during the 24 hours after surgery, or in perioperative morbidity and mortality.
Summmary • there is no evidence that thyroid hormone replacement is beneficial for patients with critical illness who have low serum T4 or T3 concentrations, or for patients undergoing CABG, whose serum T3 concentrations are known to decrease in the perioperative period. If, however, there is evidence to support a diagnosis of hypothyroidism (such as a TSH over 20 mU/L with low free T4 and/or history, symptoms, and signs of hypothyroidism), cautious administration of thyroid hormone is appropriate. RECOMMENDATIONS • Assessment of thyroid function in patients with nonthyroidal illness is difficult, especially among those hospitalized in an intensive care unit. Many of them have low serum concentrations of thyroxine (T4), free T4, and triiodothyronine (T3) and their serum thyrotropin (TSH) concentrations may also be low.
When to test • Thyroid function tests should not be measured on seriously ill patients unless there is a strong suspicion of thyroid dysfunction. • What to test • When thyroid dysfunction is suspected in critically ill patients, measurement of serum TSH alone is inadequate for the evaluation of thyroid function. Measurement of a full thyroid panel including a total T4, a free T4, and a T3 is recommended. • However, the diagnosis may still be in doubt. All methods for assessing free T4 levels are unreliable in severe critical illness; a free T4 by equilibrium dialysis sent to a reference lab would be the least likely to provide spurious results. Some experts argue a total T4 is of similar utility, at considerably less cost.
Treatment • In critically ill patients with low serum T3 and/or low T4 concentrations and no other clinical signs of hypothyroidism, we suggest not treating with thyroid hormone (Grade 2B). • In previously euthyroid patients undergoing CABG, we recommend not treating with thyroid hormone in the immediate post-operative period (Grade 1A). • If there is additional evidence to suggest a diagnosis of hypothyroidism in critically ill patients, we suggest that patients receive thyroid hormone replacement (Grade 2C). In the absence of suspected myxedema coma, repletion should be cautious, beginning with approximately half the expected full replacement dose of levothyroxine.
Sources: • Williams Textbook of Endocrinology, 12th Edition • Harrison Endocrinology, 16th Edition • UPtodate