Download
1 / 32
320 likes | 356 Views
THYROID PHYSIOLOGY AND DEVELOPMENT.

E N D
Thyrotropin-releasing hormone (TRH), a tripeptide synthesized in the hypothalamus, stimulates the release of pituitary thyroid-stimulating hormone (TSH). Pituitary TSH is a glycoprotein that stimulates the synthesis and release of thyroid hormones by the thyroid gland.
Embryogenesis begins on the floor of the primitive oral cavity, and the gland descends to its definitive position in the anterior lower neck by the end of the first trimester. Thyroid glands that do not reach the normal location are ectopic but may retain function; however, the glands most often become insufficient by early to mid childhood to support full thyroid secretion (a lingual or sublingual site or even tissue found in a thyroglossal duct cyst may be the only functioning thyroid gland). • The hypothalamic-pituitary-thyroid axis becomes functional in the second trimester. • Peripheral metabolism of thyroid hormones matures in the third trimester.
T4, triiodothyronine (T3), and TSH do not cross the placenta in significant amounts, so concentrations in fetal serum reflect primarily fetal secretion and metabolism. Antithyroid antibodies, thyroid-stimulating immunoglobulins (TSIs), iodides (including radioactive iodides), and medications given to mothers to treat hyperthyroidism (e.g., propylthiouracil and methimazole) do cross the placenta, however, and affect fetal thyroid function.
An infant born prematurely or with intrauterine growth retardation may have an interruption of the normal maturational process and appear to have hypothyroidism by standard tests. It is controversial as to whether treatment is indicated in such situations.
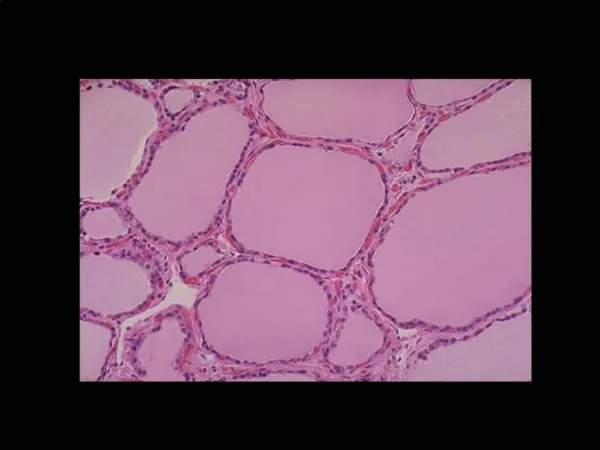
The thyroid gland (1) concentrates iodine and (2) attaches it (organifies it) to tyrosine molecules to produce either monoiodotyrosine or diiodotyrosine, with subsequent (3) coupling of two tyrosines, T4 or T3. The major fraction of circulating T3 (approximately two thirds) is derived from peripheral deiodination of T4 to T3, but some is produced by the thyroid gland itself
In Graves disease, a larger fraction originates in the thyroid gland. The conversion of T4 to T3 requires the removal of one iodine from the outer ring of tyrosine; removing an iodine from the inner ring results in reverse T3, which has little biologic effect. Preferential conversion of T4 to reverse T3 rather than T3 occurs in utero and in all forms of severe illness, including respiratory distress syndrome, fevers, anorexia, cachexia, and starvation. Conversion from T4 to T3 increases immediately after birth and throughout life.
T4 and T3 are noncovalently bound to a specific serum carrier protein, T4-binding globulin, and, to a lesser extent, albumin. Only small (<0.02%) fractions of T4 and T3 are not bound; free T4 (as it is converted to free T3) and free T3 are biologically active. Free T3 exerts metabolic effects and negative feedback on TSH release
Although a thyroid scan rarely is indicated in the evaluation of pediatric thyroid disease, the presence of thyroid agenesis or of ectopic thyroid tissue and the diagnoses of hyperfunctioning "hot" nodules or of nonfunctioning "cold" nodules may be detected by this test.
Ultrasound may determine whether it is cystic or solid. If the nodule is solid, a 123I scan indicates its functional status. Excisional biopsies usually are performed on solitary nodules. Scans are rarely indicated in the diagnosis of Hashimoto thyroiditis or thyrotoxicosis.
Hypothyroidism is diagnosed by a decreased serum free T4. Hypothyroidism might be the result of disease of the thyroid gland (primary hypothyroidism) or of abnormalities of the pituitary gland (secondary) or the result of abnormality of the hypothalamus (tertiary). Hypothyroidism is congenital or acquired and may be associated with a goiter .
Congenital hypothyroidism occurs in approximately 1 in 4000 live births and usually is caused by dysgenesis: disorders of embryogenesis (agenesis, aplasia, ectopia). Thyroid tissue usually is not palpable in these sporadic nongoitrous conditions.
The goiter reflects an inborn error of metabolism in the pathway of iodide incorporation or thyroid hormone biosynthesis or reflects the transplacental passage of antithyroid drugs given to the mother. The free T4 concentration is low, and the TSH level is elevated, proving primary hypothyroidism
Isolated secondary or tertiary hypothyroidism is rare, occurring in 1 in 100,000 live births; the free T4 is normal to low. When tertiary or secondary hypothyroidism is detected, assessment of other pituitary hormones and investigation of pituitary-hypothalamic anatomy via MRI are indicated
Although not a hypothyroid condition, congenital T4-binding globulin deficiency occurs in about 1 in 10,000 live births and is associated with a low serum total T4 concentration, a normal TSH and serum free T4, and a euthyroid status. This entity does not require treatment with thyroid hormone because it is merely a binding protein abnormality and is commonly X-linked dominant.
Newborn screening is crucial to make an early diagnosis and initiate thyroid replacement therapy by younger than 1 month of age and in the absence of definitive signs.
Findings at various stages after birth include gestation greater than 42 weeks, birth weight greater than 4 kg, hypothermia, acrocyanosis, respiratory distress, large posterior fontanel, abdominal distention, lethargy and poor feeding, jaundice more than 3 days after birth, edema, umbilical hernia, mottled skin, constipation, large tongue, dry skin, and hoarse cry. Thyroid hormones are crucial for maturation and differentiation of tissues such as bone (the bone age is often delayed at birth because of intrauterine hypothyroidism) and brain (most thyroid-dependent brain maturation occurs 2 to 3 years after birth
When treatment is initiated within 1 month or less after birth, the prognosis for normal intellectual development is excellent; screening programs usually offer therapy within 1 to 2 weeks of birth. If therapy is instituted after 6 months, when the signs of severe hypothyroidism are present, the likelihood of normal intellectual function is markedly decreased. Growth improves after thyroid replacement even in late diagnosed cases.
The dose of T4 changes with age; 10 to 15 μg/kg of T4 is used for a newborn, but about 3 μg/kg is used later in childhood. In neonatal hypothyroidism, the goal is to bring the serum free T4 rapidly into the upper half of the range of normal. Suppression of TSH is not seen in all cases and is not necessary in all cases because such suppression may lead to excessive doses of T4.
The most common cause of acquired hypothyroidism in older children in the U.S. is lymphocytic autoimmune thyroiditis (Hashimoto thyroiditis). In many areas of the world, iodine deficiency is the etiology of endemic goiter (endemic cretinism
Also known as autoimmune or lymphocytic thyroiditis, Hashimoto thyroiditis is a common cause of goiter and acquired thyroid disease in older children and adolescents. A family history of thyroid disease is present in 25% to 35% of patients, suggesting a genetic predisposition. The etiology is an autoimmune process targeted against the thyroid gland with lymphocytic infiltration and lymphoid follicle and germinal center formation preceding fibrosis and atrophy.
manifestations include a firm, nontender euthyroid, hypothyroid, or, rarely, hyperthyroid (hashitoxicosis) diffuse goiter with a pebble-like feeling; an insidious onset after 6 years of age (the incidence peaks in adolescence, with a female predominance); and sometimes a pea-sized Delphian lymph node above the thyroid isthmus. Associated autoimmune diseases include DM1, adrenal insufficiency (Schmidt syndrome), and hypoparathyroidism.
Autoimmune polyglandular syndrome type I consists of hypoparathyroidism, Addison disease, mucocutaneous candidiasis, and often hypothyroidism. Autoimmune polyglandular syndrome type II consists of Addison disease, DM1, and frequently autoimmune hypothyroidism. Trisomy 21 and Turner syndrome predispose to the development of autoimmune thyroiditis.
The diagnosis may be confirmed by serum antithyroid peroxidase (previously antimicrosomal) and antithyroglobulin antibodies. Neither biopsy nor thyroid scan is indicated in Hashimoto thyroiditis, although the thyroid scan and uptake may differentiate hashitoxicosis from Graves disease.
Treatment with thyroid hormone sufficient to suppress TSH to a normal level is indicated for hypothyroidism in Hashimoto thyroiditis. Patients without manifestation of hypothyroidism require periodic thyroid function testing (serum TSH and free T4) every 6 to 12 months to detect the later development of hypothyroidism. Goiter with a normal TSH usually is not an indication for treatment.