Download
1 / 41
410 likes | 570 Views
CDC Site Visit at Emory CHD Surveillance Cooperative Agreement Clinical & Case Finding September 25, 2013 Wendy Book, MD. Organizational Schema. Sibley Heart Center William Mahle, MD. Principal Investigator Wendy Book, MPH Co-Investigators William Mahle, MD Brian Hogan, MD

E N D
CDC Site Visit at EmoryCHD Surveillance Cooperative AgreementClinical & Case FindingSeptember 25, 2013Wendy Book, MD
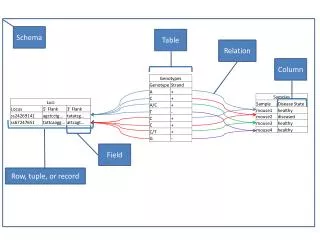
Organizational Schema Sibley Heart Center William Mahle, MD Principal Investigator Wendy Book, MPH Co-Investigators William Mahle, MD Brian Hogan, MD Carol Hogue, PhD, MPH Maan Jokhadar, PhD Michael Kramer, PhD, MPH Cheryl Raskind-Hood, MS, MPH Surveillance Database Children’s Healthcare of Atlanta Brian Kogan, MD Emory Bioinformatics Lisa Codgill Jeff Weaver Kenyon Register Andreas Kalogeropoulos Emory University Hospital Wendy Book, MD Anita Saraf, MD, PhD Emory University Hospital Midtown William Mahle, MD Emory University Rollins School of Public Health Carol Hogue, PhD, MPH Michael Kramer, PhD Cheryl Raskind-Hood, MS, MPH Grady Memorial Hospital Allen Dollar, MD Neils Engberding, MD Emory St. Joseph’s Hospital Mann Jokhadar, MD Pediatric Cardiology Services Neill Videlefsky, MD PopulationDatabase Metro Atlanta Congenital Defect Program Georgia Department of Health
Goals of RFA dd12-1207 • Determine the prevalence of CHDs among a population-based sample of adolescents and adults in the U.S.; • Describe the health care utilization and direct medical care costs for adolescents and adults with CHDs; • Describe the distribution of disease severity, co-morbidities, and longer term outcomes of adolescents and adults with CHDs; • Describe any racial/ethnic or socioeconomic disparities in healthcare use or long-term outcomes; • Monitor the health outcomes in special populations such as pregnant women with CHDs; • Calculate the survival and life expectancy for persons with specific types of CHDs; • Describe the availability of specialty care and referral patterns that are currently in place; • Assist with public health planning.
Congenital Heart Public Health Consortium (2012) “Because there is no population-based surveillance of CHD across the lifespan in the United States, no prevalence data are available on children, adolescents, and adults living with CHD.”
Adult & Children Living with CHD: Prevalence Across the Lifespan 2000 (U.S.) Estimates • 800,000 adults • 600,000 children 2010 (extrapolation based on Canadian data) to U.S. Census data in 2010 • 2 million people (all ages) were possibly living with CHD in the United States, approximately: • 975,000 to 1.4 million children • 959,000 and 1.5 million adults. Note. Data from Congenital Heart Public Health Consortium, 2012.
What’s different about Georgia? • Georgia > 3% U.S. population • Atlanta metro area has grown significantly since 1960’s - now represents > 1% of the U.S. population • However, same training structure remains – one major medical school in Atlanta, one major CTS training program, one major cardiology program • NY & MA - multiple programs Note. Data from U.S. Census 2010
Metropolitan Atlanta Congenital Defects Program (MACDP) • Established 1967 by CDC, Emory University and GMHI • Covers a 5-county metropolitan Atlanta Population of about 2.9 million, with 51,600 annual births
Provisions of Outpatient Pediatric CHD Care Outpatient • CHOA outpatient, a.k.a. Sibley Heart Center, has44 cardiologists at 19 offices • Pediatric Cardiology Services: 4 cardiologists • 4 other pediatric cardiologists • Lower CHD capture • Medical College of Georgia (Augusta) • 6 pediatric cardiologists
Provisions of Outpatient Pediatric CHD Care Atlanta Augusta Medical College of Georgia
Inpatient Pediatric Care in Georgia • Children’s Healthcare of Atlanta (3 hospitals) • >85% of care in state, majority of all care in metro Atlanta • No other children’s hospital in metro Atlanta • One other provider of inpatient pediatric care • Medical College of Georgia (Augusta)
Pediatric*Cardiac Surgical Volume by Site2008-2010 * up to age 21 ** Medical College of Georgia *** Children’s Healthcare of Atlanta
Adult Congenital Heart Care in Georgia • One Adult Congenital Heart Center in Georgia – Emory Healthcare (Emory HC) • Emory HC network is largest provider of cardiac care in Georgia • Model for transition • No patients >21 yrs. followed in the pediatric program
Other Providers of Adult CHD Care • Emory Healthcare includes St. Joseph’s • Grady Health and Grady Memorial Hospital (GMH) - more than 36,000 cardiology visits annually • Numerous private practices • Referral pattern for Adult CHD care is to Emory
Emory Adult Congenital Heart CenterVisit Numbers EHC Visits • EHC system sees 1.5 million visits per year • Nearly 250,000 unique new patients each year • EHC provides 170,000 cardiology visits per year
Age Distribution, ACHD Clinic # patients
Data Sources • Metropolitan Atlanta Congenital Defects Program (MACDP) • Linked with National Death Index (NDI) • Children’s Healthcare of Atlanta (CHOA) • Sibley Heart Center (Sibley) • Pediatric Cardiology Services (PCS) • Emory Healthcare (EHC) • Grady Health & Grady Memorial (GMH) • CMS Medicaid Data • Georgia Vital Records
Data Sources 2008-2010 • Emory Healthcare – clinical electronic medical (eMR) records (current started 2009) and archived data available (2008) • Grady Health – clinical electronic records (current started 2011) and archived electronic records (2008-2010 available) • Sibley – Current and archived data available • Pediatric Cardiology Services - electronic records • CMS Medicaid (Children’s Medical Service – previously CCS - program provided care for CHD patients up until age 21 in a Medicaid expansion program. This data was not reported to CMS. Program ended 2009) • MACDP with NDI – NDI linkage currently being revisited • GA Vital Records (Death Certificates) – provided by GA Dept. of Public Health and maintained at CDC
Georgia Population Density & Counties Georgia Population Density Clinical Surveillance Counties
Pregnancy Plan • Patient will be identified through billing codes for cardiac disease in pregnancy, cross-referenced with codes for CHD • Existing pregnancy data can be de-identified and shared, but referral bias due to clinical research set at tertiary center • Maternal mortality review (Georgia)
Surgeries, Procedures & Other Studies • Procedures – “less invasive” repairs, typically done in the cath lab in cardiology • Diagnostic Cath • Imaging studies (MRI, CT, Echo) • EKG • Map to CPT/ICD9 codes, use STS grouping?
Uninsured & MedicaidPatient Numbers • EHC • Sibley/CHOA Adolescent 11-21 years • Grady Health • Overall 4% uninsured, 5% Medicaid overall • ACHD 8% uninsured, 11% Medicaid • <5% uninsured • 47% Medicaid • 53% Uninsured • 14% Medicaid
Data: Progress to Date • Data acquired from Sibley, CHOA, EHC data warehouse • Archived EHC data received, being reviewed • IRB protocol submitted, approval is pending final DUA approvals • DUA approval required for Grady Health data • Meeting held with Pediatric Cardiology Services, expect data in next month
Challenge #1: “Out of Care” • In the “Natural History Study”, 40% of patients with AS/PS/VSD had not had a cardiac examination in over 10 years.1 • Of 10,500 adults with congenital heart disease in Germany, 8,028 were lost to follow up for more than 5 years.2 • Second natural history study of congenital heart defectsCirculation 1993 • Wacker A. Outcomes of operated and unoperated adults with congenital cardiac disease lost to follow up for more than five years. Am J Cardiol2005.
CanadianExperience Of adults with congenital heart disease transitioning to level 3 care, >25% had not had a single evaluation after their 18th birthday. Reid. Prevalence and Correlates of Successful Transfer From Pediatric to Adult Health Care Among a Cohort of Young Adults With Complex Congenital Heart Defects Pediatrics 2004
Gaps in Care: HEART-ACHD Project • 922 subjects from 12 ACHD centers. • A >3 year lapse in care identified in 42% (25% w/ severe) • 8% having lapses >10 years. • Mean age at first lapse was 19.9 years • Subjects were highly educated with 73% having more than high school education. Gurvitz M, Valente A, et al. Prevalence and predictors of gaps in care. J Am CollCardiol. 2013 May 28;61(21):2180-4
Challenge #2: Uninsured National Inpatient Hospital Database (1998-2004 & 2004-2010) • 60% of persons between 2004-2010 had public insurance or were uninsured (O'Leary, Siddiqi, de Ferranti, Landzberg, & Opotowsky, 2013) • ? accessibility of medical care to patients with public insurance or those who are uninsured • ? increasing utilization of hospital care
Self-Care Trends in ACHD • Between 40-60% of adultsare not engaged in routine care • up to 85% do not meet physical activity recommendations Dua, Cooper, Fox, & Graham Stuart, 2007 • At least 20% of women do not attend pre-pregnancy counseling despite high rates of maternal and fetal complications Bowater et al., 2012 Drenthenet al., 2007 Gurvitz, M., Verstappen, A., Valente, A.M, Broberg, C., Cook, S., Stout, K., Kay, J., Ting, J., Kuehl, K., Earing, M., Webb, G., Opotowsky, A., Graham, D., Khairy, P., Landzberg, M., 2011
Challenge #3: ICD-9CM Codes for Case Definitions • Misuse of codes • 745.5 codes for ASD and for normal variant PFO (roughly 25-30% of population) • In adults, PFO often picked up incidentally on echo for other indications • 745.4 codes for VSD. Post-myocardial infarction VSD may also be under this code (1% of fatal MI) • 552K MI fatalities per year in U.S. • MI 208 per 100,000 in 2008
The Problem: Where Are They Now?? I am 745.10
Transposition of Great Vessels:Mustard or Senning Palliation WeltonM. Gersony, CHD
This is What 745.10 Might Look Like in an Administrative Database 1969: Balloon septostomy for dTGA 1973: “Mustard” procedure, atrial switch (no code) 1990: Hospitalization: Sick sinus syndrome (427.81), Pacemaker placed (33206) 1994: Hospitalization: Heart Failure (428.0) 1999: Pregnancy complicated by heart failure (648.5) 2003: Atrial flutter (427.32) 2009: Sudden Death, Death Certificate: (I46.2)
How Do We Group CHDs? • 3 categories – Minor, Major, CHD with co-morbidities • Healthcare Utilization • By Age • By Severity • Suggestions: group by utilization & co-morbidities instead