Download
1 / 31
340 likes | 1.02k Views
Pelvic Inflammatory Disease. Does LEEP increase the risk of PTB before 37 weeks?. Compared women with history of LEEP to Women with no history of CIN or LEEP Women with history of CIN but no LEEP History of LEEP verses Group 1 RR 1.61 History of LEEP verses Group 2 RR 1.08

E N D
Does LEEP increase the risk of PTB before 37 weeks? • Compared women with history of LEEP to • Women with no history of CIN or LEEP • Women with history of CIN but no LEEP • History of LEEP verses Group 1 • RR 1.61 • History of LEEP verses Group 2 • RR 1.08 • Risks factors leading to CIN probably more important than the LEEP
Pathophysiology • Starts as cervicitis caused by GC, chlamydia, or mycoplasm • In the presence of bacterial vaginosis, there is a breakdown of mucous and other natural barriers allowing an ascending infection • Normal vaginal flora is the source of a polymicrobial infection.
Causative Agents • N. gonorrhea ▪ 20% of women with this cervicitis will develop acute PID ▪ Intense inflammatory reactions in the tubal mucosa
Causative Agents • Chlamydia ▪ More prevalent than Neisseria ▪ Clinically produces a mild for of salpingitis with an insidious onset ▪ 30% of women with this cervicitis develop PID
Type of Agent STD Endogenous agent aerobic or facultative Anaerobic Organism Chlamydia trachomatis Neisseria gonorrhea Mycoplasma hominis Streptococcus sp. Staphylococcus sp. Haemophilus sp. Escherichia coli Bacteroides, Peptococcus, Clostridium, Actinomyces Microorganisms Isolated from the Fallopian Tubes with Acute PID Weström L: Sex Transm Dis 11:439, 1984
Symptoms • Abdominal pain • Abnormal discharge • Postcoital spotting • Fever • Low back pain • Nausea/vomiting
How to approach the diagnosis? • Does she have cervicitis? • Is the cervix inflamed, tender, and/or friable? • Is the there leukocytes in the wet mount?
Mucopurulent cervicitis Mucopurulent cervicitis caused by C. trachomatis(Holmes, 1999; reprinted with permission from McGraw Hill.)
Physical Findings • Pelvic tenderness • Cervical, uterine, or adenexal • Less than 1/3 have fever • WBC commonly normal • Sed rate is generally elevated
CDC recommends treating sexually active women 25 or less years old at risk for STD if they are having pelvic or low abdominal pain AND 1) cervical, uterine, or adenexal tenderness; 2) no other causes of pain
Gonococcal Cervicitis • Recommended • Ceftriaxone 250 mg IM plus Azithromycin 1 gm po or doxycycline 100 mg po BID x 7days • Alternative regimen • Cefixime 400 mg po plus Azithromycin 1 gm po or doxycycline 100 mg po BID x 7days • If penicillin allergy • Azithromycin 2 gm po
Cervicitis Treatment Azithromycin 1 gm po x 1 OR Doxycline 100 mg bid x 7d PLUS Ceftriaxone 125 mg IM OR Cefixime 400 mg po PLUS Treat for BV if present
Indications to hospitalize… • Pregnancy • Adolescents with unpredictable compliance • Immunodeficient ( HIV with low CD4 counts) • Uncertain diagnosis • Nausea and vomiting, high fever • Inadequate response to outpatient therapy • TOA CDC .Guidelines for Treatment of Sexually Transmitted Diseases 2002, MMWR 2002: 51: 1041
Post Hospitalization Doxycycline 100 mg orally twice a day for 14 days Clindamycin 450 mg orally four time s a day for 14 days
TOA • Tubo-ovarian abscess (TOA) • collection of pus delimited by the adherence of the fallopian tubes, ovaries, and adjacent organs • serious manifestation of PID and generates 350,000 hospitalization/150,000 surgeries/yr • 34% of PID cases hospitalized have TOA • TOA ruptured -mortality rate is as high as 9% • 1-4% rupture at initial presentation or during conservative management Soper DE. Pelvic inflammatory disease. Infect Dis Clin North Am. 1994;8:821-840
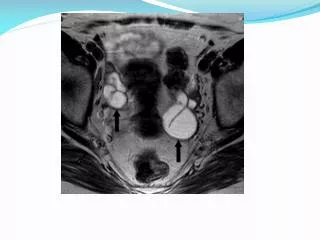
Presenting symptoms and findings with TOA Pelvic pain Pelvic mass Fever/chills Vaginal discharge Abnormal uterine bleeding Nausea/vomiting Temp.>100°F WBC>10,000 Tuboovarian abscess Pelvic inflammatory disease, proven chlamydial pyosalpinx. Right tube is swollen and tortuous (arrow) (Holmes, 1999; reprinted with permission from McGraw Hill.) Landers DV and Sweet RL: Rev Infect Dis 5:879, 1983
Diagnostic tests • Ultrasound • Complex cystic mass containing multiple septations and internal echoes • correctly identified TOA in 94% of pt. confirmed by surgery • Bulas DI. Radiology. 1992;183:435
Criteria for treatment success: • Clinical improvement may take 72 hours • Resolution of abdominal pain, defervescence, decreased WBC, stabilization or decrease in mass size. • clinically deterioration or development of an acute abdomen should prompt surgical intervention
Post Hospitalization for TO Clindamycin 450 mg orally four times a day for 14 days
Surgery • TAH/BSO • Laparoscopy with endoscopic drainage, irrigation, lysis of adhesions • Ultrasound guided percutaneous drainage
Sequelae • Chronic pelvic pain • Ectopic pregnancy • Infertility