Download
1 / 24
270 likes | 652 Views
Pelvic Inflammatory Disease. Katie DePlatchett, M.D. AM Report January 4 th , 2010. Pelvic Inflammatory Disease. An infection in the upper genital tract not associated with pregnancy or intraperitoneal pelvic operations. Anatomy 101. Epidemiology. Annual incidence: 300,000 cases

E N D
Pelvic Inflammatory Disease Katie DePlatchett, M.D. AM Report January 4th, 2010
Pelvic Inflammatory Disease • An infection in the upper genital tract not associated with pregnancy or intraperitoneal pelvic operations
Epidemiology • Annual incidence: 300,000 cases • ~20% of 1.5 million cases of GC/Chlamydia • 85% of infections are spontaneous in sexually active females. • 15% of infections develop following procedures that break the cervical mucus barrier
Risk Factors • age at first voluntary intercourse less than 18 • nonuse of barrier contraception • less than 12 years of education • more than one male sexual partner in the previous 30 days • prior gonorrhea infection • intercourse during menses
Pathogenesis Ascending infection • Along mucosa • Bacterial colonization fallopian tubes & endometrium • Chlamydia trachomatis • Neisseria gonorrhoeae
Complications • Tuboovarian abscesses • Perihepatitis, also known as Fitz-Hugh–Curtis syndrome • tubal factor infertility • ectopic pregnancy • chronic pelvic pain
Symptoms according to ACOG • Abnormal vaginal discharge • Pain in the lower abdomen (often of a mild, aching nature) • Fever and chills • Dysuria • Nausea and vomiting • Dysparunea
Diagnosis, per CDC Guidelines Minimum Criteria: • Sexually active • Lower abdominal tenderness or Adnexal tenderness or Cervical motion tenderness • No other plausible causes RoutineCriteria: • Oral temperature >38° C • Abnormal cervical or vaginal discharge (mucopurulent) • Presence of abundant WBCs on microscopy of vaginal secretions • Elevated erythrocyte sedimentation rate • Elevated C-reactive protein • Laboratory documentation of cervical infection with N. gonorrhoeae or C. trachomatis
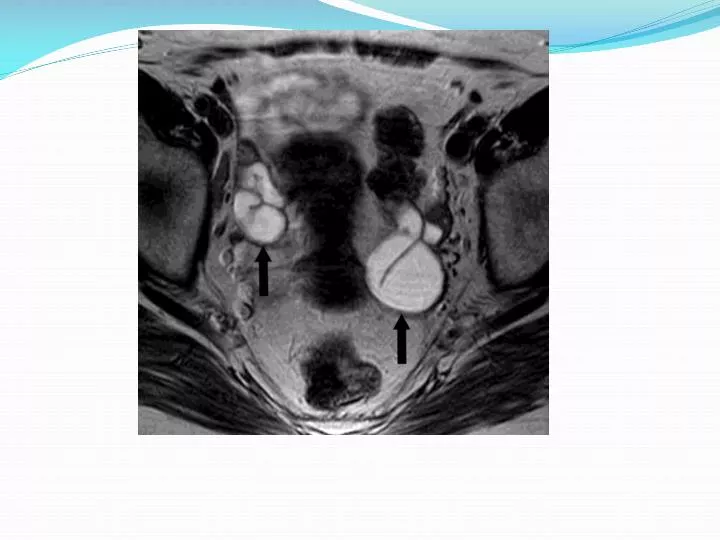
Diagnosis, per CDC Guidelines Definitive Criteria for Diagnosing PID • Histopathologic evidence of endometritis on endometrial biopsy • Transvaginal sonography or MRI showing thickened fluid-filled tubes with or without free pelvic or tuboovarian complex • Laparoscopic abnormalities consistent with PID
Diagnosis • Gold Standard = Direct visualization via the laparoscope • However… operative laparoscopy during acute infection has not been proven to reduce the prevalence of long-term sequelae. • Hence, the diagnosis of the majority of episodes of acute PID is made on the basis of clinical history and physical examination.
Imaging • Ultrasonography • sensitivity 75%–82% • helpful in documenting an adnexal mass, especially during difficult pelvic examination (tenderness or BMI) • CT • sensitivity 90%–100%
CDC Ambulatory Management of Acute PID • Levofloxacin 500 mg PO once daily for 14 days PLUS • Metronidazole 500 mg PO bid for 14 days OR • Ceftriaxone 250 mg IM in a single dose OR other parenteral third-generation cephalosporin PLUS • Doxycycline 100 mg PO bid for 14 days • Metronidazole 500 mg PO bid for 14 days
Admission Worthy • Surgical emergencies (eg, appendicitis) cannot be excluded •Pregnancy • The patient does not respond clinically to oral antimicrobial therapy • The patient is unable to follow or tolerate an outpatient oral regimen •Severe illness, nausea and vomiting, or high fever • The patient has a TOA (tuboovarian abscess)
Inpatient Treatment • Cefotetan 2 g intravenously (IV) every 12 hoursORCefoxitin 2 g IV every 6 hoursPLUSDoxycycline 100 mg orally or IV every 12 hours • “carefully monitored for an adequate response to antibiotics and any signs of rupture of the TOA and discharged after sufficient response to parenteral antibiotics is demonstrated “
Surgical Management • life-threatening infections • ruptured tuboovarian abscesses • laparoscopic drainage of a pelvic abscess • persistent masses in older women for whom future childbearing is not a consideration • removal of a persistent symptomatic mass.
Back to our patient… • Studies have demonstrated an overall 70% success rate with conservative medical management of TOAs • Success of medical management has been demonstrated to be inversely proportional to the size of the TOA. • Reed and colleagues evaluated 119 women with TOAs • >10 cm 60% required surgery • 4 to 6 cm 20% required surgery
What about IUDs?? • Increase risk in developing PID in the first month after insertion • The PID risk in IUD users is modified by: • the number of sexual partners of the IUD user and that of her partner(s) • community prevalence of STDs • age of the IUD user • Case reports of pelvic/abdominal actinomyces abscesses in IUD users , mostly out of Europe
Why Should You Care? Chronic Pain -- pelvic pain --dyspareunia -- abdominal pain
Why should you care? • Lifetime cost of $1060 to $3180 per case. • During 2008: • $15.9 billion annually spent on tx of STDs • $166 million was spent on treatment of chronic pelvic pain • $295 million was spent on treatment of ectopic pregnancies • $360 million was spent on infertility treatments as a direct result of previous PID infection.
What Can You Do? • CDC recommends : • yearly chlamydia testing of all sexually active women age 25 or younger. • Older women with risk factors for chlamydial infections (those who have a new sex partner or multiple sex partners),
References • Katz. Comprehensive Gyn, 5th Ed. 2006. • Pelvic Inflammatory Disease and Tubo-ovarian Abscess. Infectious Disease Clinics of North America - Volume 22, Issue 4 (December 2008). • Centers for Disease Control and Prevention: 2006 Guidelines for treatment of sexually transmitted disease. MMWR 55:11, 2006 • Intrauterine devices - upper and lower genital tract infections. Contraception. 2007 Jun;75(6 Suppl):S41-7. • Yeh J., Hook , III , IIIE., Goldie S.: A refined estimate of the average lifetime cost of pelvic inflammatory disease. Sex TransmDis 30. 369-378.2003 • Rein D.B., Kassler W.J., Irwin K.L., et al: Direct medical cost of pelvic inflammatory disease and its sequelae: decreasing, but still substantial. ObstetGynecol 95. 397-402.2008.